



Urinary tract stones can occur in around 12% of the population in their lifetime, and it is one of the common presentations to the emergency department.1
With the evolution of emergency medicine practices, point of care ultrasound (POCUS) has become one of the most useful inventions. POCUS is found to be 75.8% sensitive and 55.2% specific in detecting hydronephrosis secondary to obstruction in the urinary tract with the positive likelihood ratio of 1.69 in the literature.2
The most common manifestation of ureteric stone is ureteric colic or pain in the flank areas with or without radiation to the groin, which patients grade as the most severe pain of their lives.3
Case
A middle-aged female patient presented to our emergency department with the complaint of left-side abdominal pain, mild, intermittent, sharp in nature, non-radiating, and associated with one episode of vomiting for the past 6 days with no aggravating or relieving factors. Patient denies any urinary complaints or vaginal discharge or bleeding. Her last menstrual period was 1 week prior. Upon initial assessment, the patient is sitting comfortably in a chair, no signs of distress identified. Initial vital signs are normal.
On examination, there was no significant tenderness in the abdomen and no distention noted. Initial investigations revealed acute kidney injury, with a creatinine value of 91 mmol/L and high inflammatory markers including white cell count of 14.4 * 103 and c-reactive markers of 324.2 mg/L. POCUS was used to assess the underlying pathology, and revealed unexpected, severe left-side hydronephrosis [Figure 1].
Figure 1.
Urine dipstick showed 3+ leukocytes and blood; later urine culture grew Klebsiella Pneumoniae. Computed tomography scan (CT scan) demonstrated 18 mm left-side ureteric stone at S1 level [Figure 2] with perinephric fat stranding and cortical thinning.
Figure 2.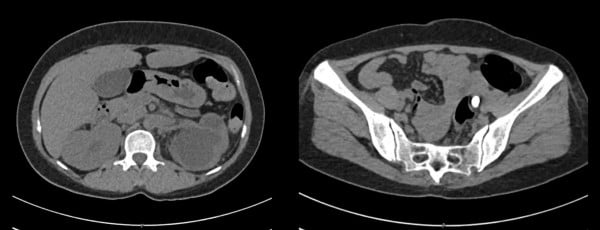
Case Conclusion
The patient was admitted under urology and underwent cystoscopy, left ureteroscopy, and left DJ stent placement. The patient was discharged home after intervention with follow up in outpatient department with urology.
TAKE-HOME POINTS
This case highlights the diversity we can get in emergency departments. It also emphasizes the importance of use of POCUS for undifferentiated or challenging cases when your initial assessment is inconclusive.
- The use of POCUS in emergency departments can be crucial in helping determine a pathology and reach a diagnosis.
- Keep differentials wide without fixating on norms or usual presentations.
References
- Teichman JM. Clinical practice. Acute renal colic from ureteral calculus. N Engl J Med. 2004;350(7):684-693.
- Al-Balushi A, Al-Shibli A, Al-Reesi A, et al. The Accuracy of Point-of-Care Ultrasound Performed by Emergency Physicians in Detecting Hydronephrosis in Patients with Renal Colic. Sultan Qaboos Univ Med J. 2022;22(3):351-356.
- Sasmaz Mİ, Kirpat V. The relationship between the severity of pain and stone size, hydronephrosis and laboratory parameters in renal colic attack. Am J Emerg Med. 2019;37(11):2107-2110.