



A 22-year-old male presented to the emergency department after an accidental fall from a motorized scooter going 20 miles per hour without wearing a helmet.
The patient states he hit a pothole, was thrown over the handlebars of his scooter, and had loss of consciousness after hitting the pavement.
On arrival, his vital signs were normal and he appeared alert and oriented to person, place, time, situation. He denied any alcohol or drug use. He appeared uncomfortable and was actively vomiting while sitting on the stretcher. The vomitus was yellow in color. A cervical collar was immediately placed due to the reported mechanism of injury. The patient was moving all four of his extremities with no difficulty and following commands. He had a right forehead abrasion, no external chest trauma, lungs clear to auscultation bilaterally, abdomen soft with no evidence of Cullen or Grey Turner sign. Elicited on exam were a positive Murphy sign and epigastric tenderness. A bedside eFAST exam was performed and was negative. All other systems were unremarkable.
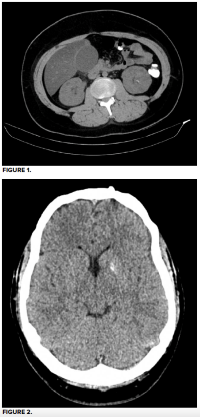
Laboratory values showed hemoglobin 13.4, creatinine 2.02, sodium 159, potassium 4.1, lactic acid 2.4, ALT 52, AST 71, total bilirubin 0.4, lipase 19, troponin < 0.01, and a small amount of blood in his urine. CT abdomen with contrast showed a dilated gallbladder with wall thickening and possible cholecystic fluid versus hemorrhage (figure 1). CT head revealed a small isolated subarachnoid hemorrhage (figure 2). A follow-up right upper quadrant ultrasound showed a heterogenous intramural fluid collection with associated wall thickening consistent with post-traumatic gallbladder hematoma (figure 4).
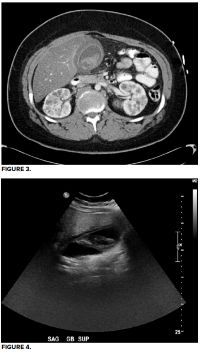
General surgery was consulted and recommended admission to their service for repeat CBC, repeat imaging, and serial abdominal examinations. On hospital day 2 abdominal tenderness resolved and diet was advanced as tolerated. Repeat CT abdomen (figure 3) and CT head showed no interval changes. On hospital day 3 liver functions tests increased to ALT 76, AST 92, total bilirubin 1.5. On hospital day 4 liver function tests and bilirubin levels normalized. Hemoglobin and creatinine remained stable throughout the hospital course, and the patient was discharged with outpatient general surgery clinic follow-up.
CASE DISCUSSION
Gallbladder injuries are most commonly caused by penetrating trauma as opposed to blunt trauma. Only 2% of gallbladder injuries are isolated, while 49% are associated with additional injuries with secondary hemodynamic instability. Traumatic isolated gallbladder hematomas are rare, with only five previously reported cases found on review of the available literature.1-5 The case above is the first reported to have been caused by an electric scooter accident. Gallbladder hematoma diagnosis is suggested by CT or right upper quadrant ultrasound. Definitive diagnosis is made by surgical exploratory laparotomy.1
Again, due to the presentation with isolated gallbladder hematoma being rarely reported, no definitive management guidelines exist. The cases discovered in our literature review and the case above were managed by serial abdominal examinations, serial imaging with CT or ultrasound, and ruling out possible complications of gallbladder injury. More than 90% of gallbladder trauma is associated with additional visceral injury. The common complications associated with gallbladder hematoma are duodenal hematoma and associated abdominal traumatic injuries. Duodenal hematoma must be ruled out when evaluating a patient for gallbladder hematoma because duodenal hematoma can lead to perforation and gastric outlet obstruction.2
CONCLUSION
Isolated traumatic gallbladder injury is extremely rare and must be thoroughly evaluated due to the complications associated with traumatic gallbladder injury. Complications such as duodenal hematoma and associated traumatic abdominal injuries must be ruled out. No definitive treatment guidelines exist but previous case reports recommend serial abdominal examinations and repeat imaging with CT and ultrasound.1,4 If the patient is hemodynamically unstable or shows no improvement in their condition, the definitive treatment is cholecystectomy or percutaneous drainage.1
Our patient had a 4-day hospital course. Hemoglobin remained at admission baseline throughout the hospital stay. Repeat CT abdomen did not reveal any significant changes in gallbladder appearance, and the patient was discharged in stable condition without complaint of abdominal pain. The patient was discharged home with outpatient surgery follow-up.
TAKE-HOME POINTS
- Isolated gallbladder injuries are incredibly rare, so high suspicion must be maintained for additional injuries.
- The most common injury accompanying a gallbladder hematoma is a duodenal hematoma.
- Duodenal hematoma can result in small bowel obstruction.
- The imaging studies of choice for diagnosis of gallbladder hematoma are CT or right upper quadrant ultrasound.
REFERENCES
- Wang IT, Tsai MT, Huang CY, et al. Isolated gallbladder hematoma after a blunt abdominal trauma: case report. Crit Ultrasound J. 2015;7(Suppl 1):A27. Published 2015 Mar 9. doi:10.1186/2036-7902-7-S1-A27
- Tudyka V, Toebosch S, Zuidema W. Isolated Gallbladder Injury after Blunt Abdominal Trauma: a Case Report and Review [published correction appears in Eur J Trauma Emerg Surg. 2008 Jun;34(3):320]. Eur J Trauma Emerg Surg. 2007;33(5):545-549. doi:10.1007/s00068-007-6202-x
- Jung YM, Son BK, Ahn SB, Kim DH, Kim EK. Intramural gallbladder hematoma mimicking gallbladder neoplasm in a 55-year-old male patient. J Korean Surg Soc. 2011;81(3):216-220. doi:10.4174/jkss.2011.81.3.216
- Jaggard MK, Johal NS, Choudhry M. Blunt abdominal trauma resulting in gallbladder injury: a review with emphasis on pediatrics. J Trauma. 2011;70(4):1005-1010. doi:10.1097/TA.0b013e3181fcfa17
- Tan SW, Lai SK, Ng KW, Chen P, Chen KH, Jiang CF. Intramural gallbladder hematoma mimicking gallbladder neoplasm in a 33-year-old male. J Chin Med Assoc. 2005;68(3):146-149. doi:10.1016/S1726-4901(09)70237-0