



Lead Author
John Paul Detherage III, MD
Chair, EMRA Sports Medicine Committee
Resident, PGY-3
Emergency Medicine
Allegheny General Hospital
Contributing Authors
Dennis Hanlon, MD, FAAEM
Associate Professor
Emergency Medicine
Drexel University COM
Mackenzie McGahan, DO
Resident, PGY-4
Emergency Ultrasound Fellowship Program
Allegheny General Hospital
Gustavo Garcia, DO
Resident, PGY-2
Emergency Medicine
Allegheny General Hospital
Mark Scheatzle, MD, MPH
Associate Professor
Emergency Medicine
Drexel University COM
Program Director
Emergency Ultrasound Fellowship Program
Allegheny General Hospital
Editors
Stephen Alerhand, MD
Assistant Professor
Emergency Medicine
Rutgers New Jersey Medical School
Director, Clinical Ultrasound Fellowship Program
Co-Director, Emergency Ultrasound Division
Louisa Weindruch, DO
Chair, EMRA Ultrasound Committee
Resident, PGY-1
Emergency Medicine
Baylor University Medical Center
History of Present Illness
A 61-year-old male presents to the emergency department after feeling a “pop” in his right knee while planting his foot playing competitive table tennis. He has no known previous injuries to his right lower extremity. The patient reports pain as well as the inability to bear weight or straighten his leg.
Physical Exam
Visual examination reveals a depression superior to the patellar pole (gap sign). He is unable to actively extend his knee against gravity or perform a straight leg raise. His distal pulses and sensation are intact.
Labs and Imaging
Radiographs and point-of-care-ultrasound (POCUS) were used to assess for any fracture or soft tissue injury. Radiographs were remarkable for a large ossicle anterior to the distal femur representing a fractured enthesophyte or superior pole patella avulsion fracture (Image 1). No laboratory analysis was performed.

Image 1: Lateral x-ray of right knee showing bony avulsion of the superior pole of the patella
POCUS Technique
POCUS was performed with a linear probe (3.0-20 MHz) using the musculoskeletal preset to evaluate the quadriceps tendon (QT). A long-axis view was obtained revealing a disruption in the tendon’s normal fascicular pattern consistent with a quadriceps tendon rupture (QTR) (Image 2). Hematoma formation is visible as an anechoic area deep to the tendon rupture. The avulsed patella appears as an irregularly shaped hyperechoic structure adjacent to the injured tendon. These findings confirmed our suspicion for QTR with avulsion of patella.
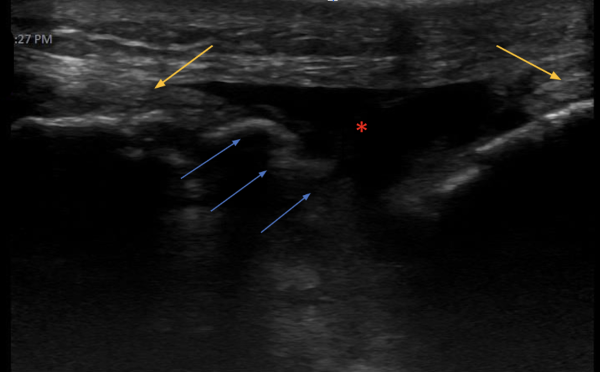
Image 2: Long axis view of the superior right knee. Asterisk (*) indicates hematoma, yellow arrows demonstrate discontinuity of the quadriceps tendon and blue arrows demonstrate hyperechoic patellar avulsions.
To perform POCUS of the quadriceps tendon, have the patient supine in a position of comfort with the knee slightly flexed, using a rolled towel posteriorly for support. Use the high frequency linear probe and select the musculoskeletal preset. To optimize the image, further adjustments can be made to the depth and gain. The structure of interest, in this case the QT, should be evaluated in both the axial and longitudinal plane.1
The axial view is obtained with the probe marker to the patient's right, starting three quarters of the way down the patient's thigh and from there sliding the probe down to the patella (Image 3). The fibrillar echotexture of four muscle structures of the quadriceps, including the rectus femoris, vastus lateralis, vastus intermedius and vastus medialis, is initially visualized. The four muscle bellies are visualized converging into the QT as the probe is slid distally to the patella.

Image 3

Image 4
To obtain the longitudinal view, begin scanning in the same location as the axial view with the probe rotated 90 degrees with the probe marker facing cephalad. Slide the probe caudally until the insertion site into the patella is visualized. Healthy tendons have a striated appearance with multiple, closely spaced hyperechoic parallel lines with echogenicity distinct from the surrounding soft tissue. Disorganized-appearing fibers are suspicious for tendon injury. Hypoechoic or anechoic areas within the tendon represent disruption of the fibers, bleeding or hematoma formation which are also indicative of tendon injury.
In the longitudinal view, it is important to have the probe perpendicular to the tendon. If not completely perpendicular, hypoechoic areas may appear within the tendon leading to a false positive result. This phenomenon is known as anisotropy.2 The integrity of the QT may also be examined dynamically by having the patient attempt to extend the knee while directly visualizing the tendon in the longitudinal axis. After thorough investigation of the QT, use the same technique to visualize the patellar tendon, evaluating its course from the patella to insertion into the tibial tuberosity.
To complete the exam, examine the patient’s non-injured knee and compare findings. A normal QT is shown in the axial view (Video 1) and longitudinal plane (Videos 2 and 3).
Video 1
Video 2
Video 3
(Video Clips Provided by Stephen Alerhand, MD)
Discussion
QTR is rare, with an estimated incidence of 1.37 cases per 100,000 people/year, typically occurring in patients 40 years of age or older after sudden changes in direction or jumping and landing.3 Early diagnosis and surgical repair along with a strong rehabilitation program correlate to better outcomes.4
Although MRI is the gold standard for diagnosing complete QTR, this is not always practical in the ED. POCUS is a time-efficient, economical approach to assessing acute knee injuries, especially when evaluating the integrity of tendons.5 However, patients may require MRI for definitive diagnosis and operative planning, as ultrasound has been reported to have false positive results in obese and muscular patients.6
As with any POCUS, results are operator-dependent, and false-positives may result from factors such as anisotropy or inability to visualize the injured area of tendon. Therefore, POCUS is most appropriately used in conjunction with a physical examination (e.g., straight leg raise, “gap sign”), radiographs, and consideration of MRI.
In this patient, we identified QT disruption, hematoma, and bony avulsion of the patella with POCUS.
Hospital Course/Resolution
The patient was placed in a knee immobilizer and followed up with an orthopedic surgeon within 1 week.
References
- Pasta, G., et al. “Sonography of the Quadriceps Muscle: Examination Technique, Normal Anatomy, and Traumatic Lesions.” Journal of Ultrasound, vol. 13, no. 2, June 2010, pp. 76–84, https://doi.org/10.1016/j.jus.2010.07.004.
- Secko, Michael, et al. “Ultrasound Diagnosis of Quadriceps Tendon Tear in an Uncooperative Patient.” Journal of Emergencies, Trauma and Shock, vol. 4, no. 4, 2011, pp. 521–522, www.ncbi.nlm.nih.gov/pmc/articles/PMC3214514/, https://doi.org/10.4103/0974-2700.86652.
- Pope, Jacob D., et al. “Quadriceps Tendon Rupture.” PubMed, StatPearls Publishing, 2023, ncbi.nlm.nih.gov/books/NBK482389/#:~:text=Quadriceps%20tendon%20ruptures%20are%20due.
- Arnold, Evan P., et al. “Acute Quadriceps Tendon Rupture: Presentation, Diagnosis, and Management.” JBJS Reviews, vol. 10, no. 2, Feb. 2022, https://doi.org/10.2106/jbjs.rvw.21.00171. Accessed 18 Apr. 2022.
- Friedman, L., et al. “Ultrasound of the Knee.” Skeletal Radiology, vol. 30, no. 7, 1 July 2001, pp. 361–377, https://doi.org/10.1007/s002560100380.
- Swamy, Girish, et al. “Is Ultrasound Diagnosis Reliable in Acute Extensor Tendon Injuries of the Knee?” Acta Orthopaedica Belgica, vol. 78, no. 6, 1 Dec. 2012, pp. 764–70.