


Flood syndrome is defined as a spontaneous rupture of an umbilical hernia leading to sudden loss of ascitic fluid. It is a rare condition that carries a high mortality rate.
We present a case outlining the history of present illness, physical exam, laboratory data, emergency department management, and definitive treatment of one patient. There is a scarcity of literature recommending a standardized emergency department workup for Flood syndrome. We will outline a proposed approach, as well as the importance of correct and timely disposition.
Case
A 64-year-old male with a history of alcohol abuse and resultant severe cirrhosis presented to the emergency department with a chief complaint of “stomach leaking” 2 hours after noticing a yellow fluid beginning to drain from his umbilicus. His cirrhosis had been complicated by recurrent ascites requiring regularly scheduled paracentesis. His previous scheduled paracentesis was 2 months prior; during this time, he had noticed a progressive protrusion of his navel along with worsening bilateral lower extremity swelling and exertional dyspnea. The patient and his family estimated that he had lost at least 1-2 liters of this fluid prior to his arrival to the emergency department.




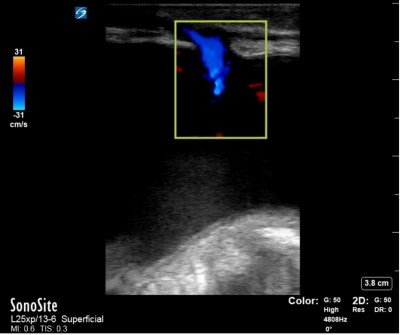
Initial vital signs revealed a blood pressure of 139/89 mm Hg, heart rate of 97 bpm, a respiratory rate of 16 breaths per minute, an oral temperature of 97.9 °F, and an oxygen saturation of 100% on room air. His physical exam was notable for severe abdominal distention with a fluid wave. The umbilicus was protuberant, and there was a small central ulceration with a large amount of clear yellow fluid slowly draining out. No tenderness, guarding, or rebound was appreciated. Bedside ultrasound showed free fluid in the abdomen with a sinus tract leading from the peritoneum to the umbilicus through a defect in the anterior abdominal wall (Ultrasound Figures 1, 2, 3). An ostomy bag was placed over the lesion and an additional liter of ascitic fluid was observed to drain spontaneously during the patient’s 5-hour stay in the ED.

Ultrasount Figure 1

Ultrasound Figure 2
Ultrasound Figure 3
Laboratory results were remarkable for a hemoglobin of 11.1 gm/dL, platelets 53 K/mm3, total bilirubin 1.2 mg/dL, albumin 3.0 g/dL, aspartate aminotransferase 32 (5-34 U/L reference range), alanine aminotransferase 12 U/L, creatinine 1.0 mg/dL, prothrombin time 16.5 seconds, and international normalized ratio 1.33.
A diagnosis of early Flood syndrome was made; albumin and IV antibiotics were administered to the patient, and general surgery was consulted for admission and definitive repair. The following day, the patient was taken for herniorrhaphy, where a 5 cm defect was identified and closed; there was no bowel incarceration or strangulation; 2.9 liters of ascites were drained intraoperatively. There were no immediate surgical complications. On postoperative day 1, the patient underwent repeat paracentesis with an unremarkable fluid analysis. He was continued on his home furosemide, spironolactone, lactulose, rifaximin, and labetalol during his hospital stay and was discharged home on postoperative day 2 with scheduled hepatology follow-up.

Post-op
Discussion
Flood syndrome (named for Frank B. Flood, who published the first case series) involves the sudden drainage of ascitic fluid from a spontaneously ruptured umbilical hernia in patients with severe liver disease. Twenty percent of patients with cirrhosis will have an umbilical hernia, and nearly half of these patients will require emergency surgery for complications related to the hernia.3 The etiology of Flood syndrome is multifactorial; contributing factors include umbilical vein dilation and varices secondary to portal hypertension, deconditioning and atrophy of abdominal musculature, poor nutritional status, and chronically elevated intra-abdominal pressure.8 The clinical course can be complicated by spontaneous bacterial peritonitis (SBP), skin and soft tissue infections, sepsis, and bowel herniation, incarceration, and strangulation. Cutaneous ulceration over the umbilicus is a warning sign that indicates impending rupture.5
No standardized treatment guidelines have been formalized for Flood syndrome. Most surgeons are apprehensive to take patients with cirrhosis to the operating room, as they carry high mortality rates and are at high risk for postoperative complications. Many of these patients present on varying spectrums of their disease course, requiring counseling on operative risks. One study gave a 13% mortality risk in the operating room for patients undergoing urgent operative repair of flood syndrome.10 Palliative care discussion may be beneficial in defining the patient’s goals of care.
The mortality of Flood syndrome patients has been shown to be reduced by 6-20% with operative repair.4Furthermore, the literature shows a 60-87% mortality rate in patients who are managed only conservatively (e.g., ostomy bag dressing, bedside closure, fibrin skin glue).4,10 Closure in the OR should be pursued if possible.5,7,13Postoperative control of ascites is essential to limit complications and recurrence.3,6,9,10 The literature has described liver transplant, TIPS procedure, pigtail catheter drains, and therapeutic paracentesis in the perioperative setting. The decision is guided by risk stratification using measures such as the Model for End-Stage Liver Disease (MELD) and Child-Turcotte-Pugh scores.
These patients should be managed closely by an interdisciplinary team. Perioperative optimization prior to surgery is essential to reducing mortality, provided there is no indication for emergent surgery.3,8,10 This includes improving nutritional status, optimizing volume status, correcting electrolyte abnormalities and coagulopathy, replacing albumin, diagnosis of SBP, antibiotics as needed, treatment of hepatic encephalopathy, and arranging postoperative control of ascites.10
It is essential that emergency medicine providers promptly recognize and correctly manage Flood syndrome as it carries a high mortality rate with delays in treatment. Disease severity and practice location may influence the need for transfer, admission, and intervention. Timely consultation with a surgeon is critical. Rural and remote emergency departments without surgical coverage should arrange for transfer to a center with higher level of care. Severity of illness presentation and associated complications should be considered and investigated.
An example workup is outlined below:
- Complete blood count, complete metabolic panel, coagulation studies, lactic acid, infectious workup including blood cultures (as directed by H&P)
- Diagnostic paracentesis. Send fluid for cell count with differential, gram stain, culture, glucose, LDH, and total protein.
- Consideration should be made for therapeutic paracentesis (with albumin repletion as needed), or pigtail catheter placement if transfer or intervention will be delayed.2
- Administer empiric intravenous antibiotics with broad-spectrum coverage.
- Determine fluid status and act accordingly (with diuresis or fluid repletion).
- Correct electrolyte abnormalities, coagulopathy, hypoalbuminemia, and thrombocytopenia as needed.
- Apply a sterile dressing or ostomy pouch over the lesion.2
- Consult general surgery and an appropriate medical service (e.g., internal medicine, gastroenterology, or hepatology).
- Admit or transfer to a facility with the appropriate level of care.
Of course, these outline some basic steps for workup in the emergency department for optimal patient outcomes. This may not be an all-encompassing or adequate list depending on clinical context and practice location.
Conclusion
Patients with cirrhosis complicated by ascites may develop abdominal wall hernias due to chronically elevated intra-abdominal pressures and weakening of the abdominal musculature. Acute care providers should be aware of the complications of umbilical hernias in patients with cirrhosis, as their perioperative mortality is high. It is crucial that all cirrhotic patients with umbilical hernias be evaluated for potential surgical repair to prevent life-threatening complications.3,5,10
References
- CASE REPORT| VOLUME 1, ISSUE 1, P5-6, JANUARY 01, 2015. Flood syndrome. Ilana J. DeLuca, MD, PhD, Marc E. Grossman, MD. Open AccessDOI:https://doi.org/10.1016/j.jdcr.2014.09.003 https://www.jaadcasereports.org/article/S2352-5126(14)00005-8/fulltext.
- Perm J. 2017; 21: 16-152. Published online 2017 Jun 26. doi: 10.7812/TPP/16-152 PMCID: PMC5499604. PMID: 28678688. Emilie T Nguyen, MD. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5499604/ Summary: pigtail cath placement, not surgical candidate.
- International Surgery Journal. Colbran R et al. Int Surg J. 2019 Oct;6(10):3830-3833. http://www.ijsurgery.com. pISSN 2349-3305 | eISSN 2349-2902. DOI: http://dx.doi.org/10.18203/2349-2902.isj20194450. Case Report Spontaneous umbilical hernia rupture with omental evisceration and Flood syndrome. Rachel Colbran1,2*, Alison Smith1, Aemelia Melloy1, Ramesh Iyer1. https://mail.ijsurgery.com/index.php/isj/article/download/4837/3247. Summary, take away points: 20-40% of cirrhosis patients will have umbilical hernias. Half require emergency surgeries for complications, thus should have operation before. This patient had a 14 day ICU stay complicated by encephalopathy, PNA, and worse ascites. Perioperative optimisation is best.
- Chatzizacharias N, Bradley J, Harper S, Butler A, Jah A, Huguet E, et al. Successful surgical management of ruptured umbilical hernias in cirrhotic patients. World J Gastroenterol. 2015;21:3109-13. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4356934/. Summary, take away points: 60-80% mortality if flood syndrome is managed supportively vs 6-20% with surgical repair. umbilical herniorrhaphy without mesh or primary closure is procedure of choice. This reduces mortality rate up to 20%.
- A rare case of Flood syndrome in emergency department: A case report and review of recent reported cases. Daniel Weei Jang Tan, Jing Jing Chan. First Published November 26, 2020 Case Report. https://doi.org/10.1177/1024907920973556.https://journals.sagepub.com/doi/full/10.1177/1024907920973556. Summary, take away points: bedside closure with drain placed resulted in eventual peritonitis. Surgical repair of all umbilical hernias in cirrhotic patients is crucial.
- A Rare Case of Flood Syndrome and a Perspective on Management. 2293 Fasullo, Matthew DO1; Oranefo, Justice MD2. Author Information. American Journal of Gastroenterology: October 2017 - Volume 112 - Issue - p S1256. https://journals.lww.com/ajg/Fulltext/2017/10001/A_Rare_Case_of_Flood_Syndrome_and_a_Perspective_on.2294.aspx. Summary, take away points: pt had TIPS then hernia repair. This reduces post surgical complications after hernia repair.
- A Case of Flood Syndrome: To Operate or Not to Operate? 2360. Singh, Sanmeet MD1; Skef, Wasseem MD1; Thaker, Sarang MD, MS2; Chan, Christine MD3. Author Information. American Journal of Gastroenterology: October 2018 - Volume 113 - Issue - p S1322. https://journals.lww.com/ajg/Fulltext/2018/10001/A_Case_of_Flood_Syndrome__To_Operate_or_Not_to.2359.aspx. Summary, take away points: presents with flood and SBP. Not TIPS or Tx candidate. Urgent abd surgery associated with better outcomes.
- Flood Syndrome: A Rare and Fatal Complication of Umbilical Hernia in Liver Cirrhosis. Cureus. 2020 Aug; 12(8): e9915. Published online 2020 Aug 21. doi: 10.7759/cureus.9915. PMCID: PMC7505645. PMID: 32968577. Monitoring Editor: Alexander Muacevic and John R Adler. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7505645/ Summary, take away points: etiology of flood is from weakened wall muscles, umbilical vein dilation, and high intraabdominal pressure. Medical plus surgical timing is key. pt had nonmesh urgent herniorrhaphy repair complicated by AKI, spontaneous pneumo and failure to thrive.
- International Journal of Medical Science and Health Research. Vol. 2, No. 04; 2018. ISSN: 2581-3366. Flood Syndrome: Rare Case Report of Ruptured Umbilical Hernia Expressing Ascitic Fluid in Liver Cirrhosis. Mr Lava Krishna Kannappa, MBBS, MRCS, Dr Mohsin Hussein, MBBS, Dr May Hnin Lwin Ko, MBBS, Mr Yahya Salama, FRCS. http://ijmshr.com/uploads/pdf/archivepdf/2020/IJMSHR_02_71.pdf. Summary, take away points: resuscitate first with fluid, abx, and plan for post op ascites managed by GI. Pt had primary repair without mesh and drain placed in OR. No complications.
- Lemmer JH, Strodel WE, Knol JA, Eckhauser FE. Management of spontaneous umbilical hernia disruption in the cirrhotic patient. Ann Surg. 1983;198(1):30-34. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC1352927/pdf/annsurg00125-0044.pdf. Summary: skin changes predicts impending rupture. 13% mortality rate in OR during urgent repair. 87% in their study in pts without operation died. Optimize prior to surgery if possible. This is associated with better outcomes and allows time to improve nutritional status, volume replacements, coagulopathy, electrolyte abnormalities, and control ascites. Stabilize with abx, sterile dressing, IV, etc. Ideally fix hernia before complications (flood syndrome) arise.
- Case Report J Med Cases. 2019;10(10):309-311Acute Abdomen From Umbilical Hernia Rupture to Flood Syndrome: A Case Report and Review of Literature. Gavin Fang Liua, d, Aswin Srinivasana, Sangeeta Mutnurib, Muralidhar Reddy Yerramadhac, Mahendra Agraharkarb. https://www.journalmc.org/index.php/JMC/article/view/3375/2675. Summary: no surgeon would operate, non-operative management lead to - cellulitis of hernia, frequent admissions for SBP and ascites, renal failure, hyponatremia.
- A Rare Case of Spontaneous Umbilical Hernia Rupture- Flood Syndrome. 1888. Azeem, Ali MD1; Latif, Summaya MD1; Pervez, Asad MD2. American Journal of Gastroenterology: October 2016 - Volume 111 - Issue - p S903-S904.https://journals.lww.com/ajg/Fulltext/2016/10001/A_Rare_Case_of_Spontaneous_Umbilical_Hernia.1888.aspx. Summary: tx course - abx, CT, Primary open surgical repair with JP drain placement.
- Flood Syndrome, a Rare Complication of Cirrhosis. Gil, Arcelia Guerson MD1; Rockwell, Bradley MD1; Galen, Benjamin MD1. The American Journal of Gastroenterology: October 2019 - Volume 114 - Issue - p S1309. doi: 10.14309/01.ajg.0000598928.69844.26. https://journals.lww.com/ajg/Abstract/2019/10001/2349_Flood_Syndrome,_a_Rare_Complication_of.2350.aspx. Summary: Non-surgical management is not advised and associated with higher mortality.
- IMAGES IN EMERGENCY MEDICINE| VOLUME 62, ISSUE 4, P431, OCTOBER 01, 2013. Man With Rushing Fluid From His Umbilicus. William D. Long, MD, Geoffrey E. Hayden, MD. DOI:https://doi.org/10.1016/j.annemergmed.2013.02.026. https://www.annemergmed.com/article/S0196-0644(13)00204-7/fulltext.