



Case
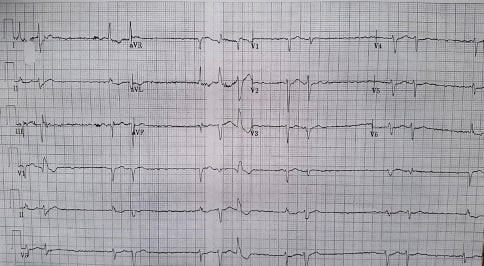
A 65-year-old female with a history of atrial fibrillation presents to the emergency department with altered mental status, weakness, and decreased oral intake. What is your interpretation of her ECG?
Answer
This ECG shows an irregular rhythm with an average ventricular rate of 70 bpm, no obvious p-waves or flutter waves, left axis deviation, and variable QRS complex duration. There are 2 and 3-beat groups of QRS complexes with the QRS complex duration increasing between beats except for the 5th group which does the opposite. The RR intervals between the 1st, 3rd, 5th, and 8th QRS complexes are somewhat consistent but then vary for the remainder of the ECG.
Discussion
The presence of repeating groups of beats should prompt consideration of a 2nd degree AV block, but this is ruled out by the absence of p-waves. Other possibilities include a junctional rhythm with PJCs or PVCs, atrial fibrillation with PJCs or PVCs, and hyperkalemia.
The presence of a slow rhythm suggests decreased or blocked AV node conduction, and the frequent premature beats suggests increased automaticity. Given the patient’s history of atrial fibrillation, these findings are concerning for digoxin toxicity.
In general, atrial fibrillation is not an intrinsically slow rhythm in the absence of a diseased or poisoned AV node. Digoxin works as a negative chronotrope by increasing the vagal effects at the AV node to slow conduction. Too much digoxin can lead to severe bradydysrhythmias and AV blocks. The initial portion of this ECG looks like atrial fibrillation with an underlying regular junctional rhythm suggestive of a 3rd degree AVB, which is one of the “classic” dysrhythmias seen with digoxin toxicity. Digoxin also works as an inotrope by increasing intracellular calcium, which can lead to increased automaticity and the presence of frequent premature beats as seen in the case ECG.
Digoxin toxicity can present with a range of bradycardias, tachycardias, and various blocks. Common dysrhythmias include paroxysmal atrial tachycardia with variable block and bradycardic rate, accelerated junctional rhythms, bidirectional ventricular tachycardia, and atrial fibrillation with slow ventricular response or a regular bradycardic rate due to the presence of a 3rd degree AV block.
Common causes of chronic digoxin toxicity include renal disease, electrolyte abnormalities, dehydration, and drug interactions. Common symptoms seen with chronic toxicity include anorexia, abdominal pain, nausea, and CNS symptoms (eg, AMS).
Digoxin effect, also called the “Salvador Dali” sign, describes the ECG features seen with digoxin use and include scooped ST-segments, prolonged PR intervals, and shortened QT intervals. Note that these ECG changes are seen with digoxin use and are not a marker of toxicity. It is also important to note that patients can have digoxin toxicity clinically with normal serum concentrations, especially in the presence of hypomagnesemia, hypokalemia, and/or hypercalcemia.
Case Conclusion
The patient’s labs were notable for an acute kidney injury and elevated digoxin level. Treatment with hemodialysis was initiated due to the severity of the patient’s renal dysfunction and concurrent digoxin toxicity. Typical first-line treatment for symptomatic dysrhythmias is digoxin immune Fab (eg, Digibind or DigiFab). This will cause potassium to shift into the cells and can lead to clinically significant hypokalemia, so potassium levels should be monitored closely after administration. It will also cause serum digoxin levels to rise making repeat levels unreliable.
Digoxin Learning Points
General Features
- Includes cardiac glycosides (eg, digoxin and digitalis derivatives, foxglove, oleander, lily of the valley, and secretions from Bufo toad spp.)
EKG Features
- Digoxin effect seen with therapeutic levels:
- Scooped ST-segment most pronounced in leads with tall R-wave (digoxin effect)
- PR lengthening
- QT shortening
- Toxicity can cause almost any dysrhythmia, including:
- Atrial fibrillation with slow ventricular response or a regular bradycardic rate
- Paroxysmal atrial tachycardia with variable block and bradycardic rate (uncommon)
- Bidirectional ventricular tachycardia (very rare)
Clinical Significance
- Acute toxicity may present with hyperkalemia
- Treatments include:
- Digoxin-specific antibody
- Atropine for AV blocks
- Phenytoin or lidocaine for ventricular dysrhythmias