



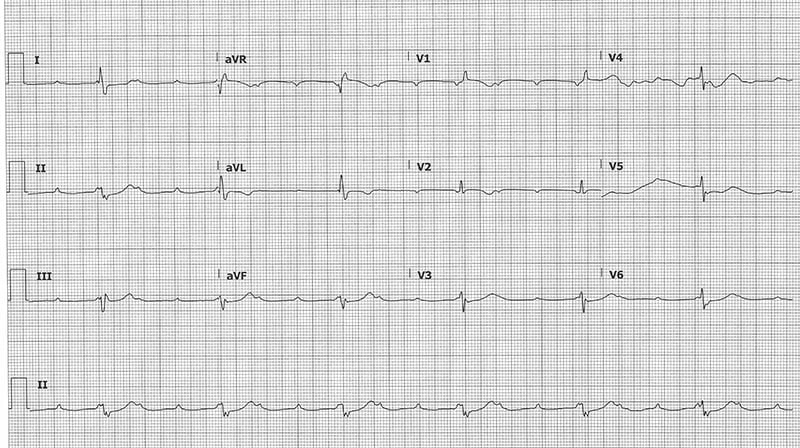
A 71-year-old female with history of aortic stenosis s/p transcatheter aortic valve replacement (TAVR) 3 days ago presents to the emergency department because of a syncopal episode earlier in the morning. What is your interpretation of her ECG?
Answer
This ECG shows a 3rd degree AV block with a ventricular rate of 38 bpm, an atrial rate of 115 bpm, left axis deviation, and a prolonged QRS duration with a RBBB.
The key to interpreting this ECG is identifying the P-waves partially buried in the initial portion of the QRS complexes (see purple down-arrows in Figure 1). The rhythm is regular with 3 P-waves for every QRS complex, which narrows the possibilities to a 3:1 AV block or a 3rd degree AV block.
Fig. 1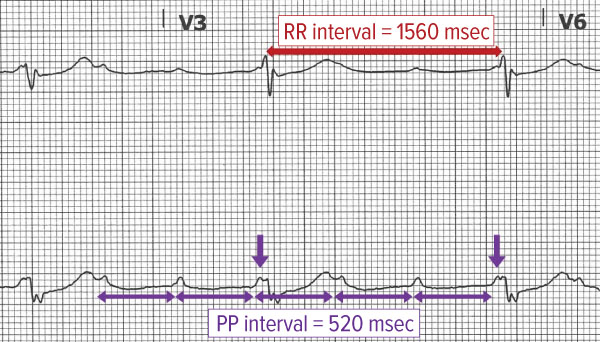
High-grade AV blocks, also called advanced AV blocks, describe when ≥ 2 sequential P-waves are not conducted. These blocks are most commonly a variant of a Mobitz type II but can be associated with a Mobitz type I. Since there are no sequential conducting P-waves to compare PR intervals, it is often impossible to determine if the underlying pathology is a Mobitz type I or type II. Note that while a wide QRS complex suggests an underlying Mobitz type II, it can also be seen with a Mobitz type I if there is a fixed or rate-related bundle branch block (eg, the patient has a bundle branch block at baseline). As well, a narrow QRS complex is not specific for an underlying Mobitz I, as it can be present in a Mobitz type II.
A 3rd degree AV block, or complete heart block, is defined by the absence of conduction through the AV node leading to complete AV dissociation. The atria and ventricles will typically march out at different rates, with the atrial rate being faster than the ventricular rate. Ventricular pacing can occur anywhere distal to the block, including the AV junction, the bundle of His, or a ventricular focus. Junctional escape rhythms typically produce a ventricular rate of 40-60 bpm and the QRS complex can be narrow in the absence of aberrant conduction. In contrast, ventricular escape rhythms typically result in rates of 20-40 bpm with a wide QRS complex.
This ECG shows an atrial rate that is 3 times the ventricular rate (see purple and red horizontal arrows in Figure 1), which suggests a 3:1 AV block. Note that the P-waves immediately preceding the QRS complexes (see purple down arrows in Figure 1) are partially buried in the QRS complexes, which means they are occurring at almost the same time. Accordingly, the QRS complexes cannot be due to normal conduction from the preceding P-waves, which points against the diagnosis of a 3:1 AV block. This suggests the presence of a 3rd degree AV block that coincidentally has an atrial rate that is 3 times the ventricular rate. Ultimately, differentiating between these two diagnoses is academic, since both warrant admission for evaluation for placement of a pacemaker.
Case Conclusion
The patient's initial ECG in the ED (not shown) demonstrated normal sinus rhythm with a right bundle branch block. The case ECG was obtained when the patient reported dizziness after getting up to walk to the bathroom (note: serial ECGs are almost never a bad idea). A few minutes after obtaining the case ECG, the patient spontaneously converted back to sinus rhythm. The patient was admitted to the Cardiac ICU for placement of a permanent pacemaker.
3rd Degree AV Block Learning Points
- A 3rd degree AV block, or complete heart block, is defined by the absence of conduction through the AV node leading to complete AV dissociation
- P-waves "march out" (constant PP interval) and do not conduct to produce a QRS complex
- PR intervals are variable
- Atrial rate > ventricular rate
- Ventricular rhythm is usually junctional or ventricular escape rhythm
- Etiologies include ischemia/infarction (often seen with inferior MI), hyperkalemia, endocarditis, drug-related (eg, AV nodal blocker toxicity, digoxin toxicity)
- Symptoms can include syncope/presyncope, DOE, chest pain, generalized fatigue
- Treatment includes:
- Transcutaneous or transvenous pacing if unstable
- All patients require admission and evaluation for pacemaker placement
High-grade (or advanced) AV Block Learning Points
- 2nd-degree AVB with ≥ 2 sequential non-conducted P-waves
- Most commonly a variant of a Mobitz type II but can be associated with a Mobitz type I
- PP and RR intervals should have a whole number ratio
- Named as ratio of P-waves to QRS complexes (ie, 3:1, 4:1, etc.)
- Can be seen after anterior MI or with significant pathology of the conduction pathway
- High risk of progressing to a 3rd degree AV block