



Syncope can have many causes that are not always evident at the initial presentation.
Case Presentation
An 80-year-old male presented to the ED following a syncopal episode with a ground-level fall. According to the patient's family, the patient was his usual self before he lost consciousness while walking within their home. The patient reportedly remained unconscious for an unknown length of time with no jerking movements, loss of bladder function, or post-awakening confusion.
Upon arrival to the ED, the patient was found to have intermittent heart rates in the 15-20s with rebound to the 50s-60s. During the bradycardic episodes, he was symptomatic with dizziness. The patient was otherwise hemodynamically stable. He denied the use of cardiovascular medications but reported an increase in pyridostigmine dosage for his myasthenia gravis approximately 2 months ago. He was admitted to Cardiology with plans for urgent pacemaker implantation.
Discussion
When considering the etiology of syncope, the differential can be categorized into reflex, orthostatic, and cardiac causes. The origin of a reflex-based syncope is most commonly vasovagal secondary to a trigger, such as stress or prolonged standing. It can also be situational, such as carotid sinus hypersensitivity.1 Orthostatic causes can be another origin of syncope and may be the result of hypovolemia, autonomic dysfunction, or the use of certain medications like vasodilators or inotropic/chronotropic blockers. Finally, cardiac syncope is syncope secondary to malfunction of the cardiovascular system and can include bradycardia, tachycardia, and structural diseases such as hypertrophic cardiomyopathy, ischemia, or valvular dysfunction.2
In this case, the patient's syncope was most likely cardiac in nature given his symptomatic bradycardia upon presentation to the ED. Initial management of symptomatic bradycardia is dependent on the patient's hemodynamic stability. If vital organ function is acutely impaired, then atropine is the initial treatment of choice. If bradycardia persists with the use of atropine, then sympathetic beta-1 stimulating medications, such as epinephrine or dopamine, may be indicated with the initiation of transcutaneous pacing if symptoms continue.3
In a hemodynamically stable patient, management becomes directed toward determining and treating the underlying cause of the bradycardia. In many cases it is due to sinus node dysfunction, acute myocardial ischemia, or medication toxicity; however, it is also important to consider non-cardiac causes of bradycardia in the differential.4
Herpes simplex virus (HSV) encephalitis is an acute central nervous system infection associated with significant morbidity and mortality. It often presents with a prodromal phase of fever, malaise, headache, and nausea followed by more severe neurologic symptoms such as meningismus and seizures.5 In rare cases, HSV encephalitis has also been shown to cause sinus node dysfunction and arrest.6
Diagnosis of HSV encephalitis can be through lumbar puncture, which most often shows pleocytosis of cerebral spinal fluid with lymphocytic predominance and elevated protein. Brain CT (Image 1) or MRI can also be used as a diagnostic tool displaying temporal lobe abnormalities.7
Image 1. CT revealing signs of CNS dysfunction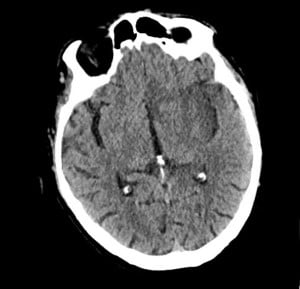
Early identification and treatment with intravenous acyclovir is crucial, as the disease carries significant rates of morbidity and mortality. Mortality is predicted to be 20-30% with prompt diagnosis and treatment but can be up to 70% for untreated infection.8 Long-term morbidity may include significant cognitive and behavioral disability including anterograde amnesia, Klüver Bucy syndrome, and seizures. When considering cardiac impairment from HSV, a previous case suggests prompt treatment may be sufficient to reverse disease-associated sinus node dysfunction without the need for permanent pacemaker implantation.9
Hospital Course
Several hours after admission, the patient underwent uncomplicated dual chamber pacemaker placement with plans to be discharged in the morning. However, upon examination the following day, the patient was displaying both expressive and receptive aphasia with right leg weakness. Workup for a possible ischemic event, seizures, or delirium revealed a negative non-contrast head CT, CTA head and neck, and cerebral perfusion imaging. Meanwhile, the patient began experiencing respiratory distress with SpO2 in the high 80s. A chest x-ray showed pulmonary vascular congestion.
With rapidly deteriorating neurological and respiratory status, the patient was transferred to the ICU and intubated. Given the deterioration of neurological status, a lumbar puncture revealed xanthochromic cerebral spinal fluid with elevated protein, elevated RBCs, and normal WBCs with elevated neutrophil fraction. HSV encephalitis was suspected at this point, and the patient was started on acyclovir. PCR results later confirmed HSV.
Conclusion
Syncope can have many causes that are not always evident at the initial presentation. As evidenced by this case, HSV encephalitis can have a variety of presenting signs and symptoms that may not appear to be of neurological origin. Clinicians should be cognizant of this variability and consider that acute CNS infections, such as HSV, may be an etiology for sinus node dysfunction in cardiac syncope patients.
References
- Moya A, Sutton R, Ammirati F, et al. Guidelines for the diagnosis and management of syncope (version 2009). Eur Heart J. 2009;30(21):2631-2671.
- da Silva RMFL. Syncope: epidemiology, etiology, and prognosis. Front Physiol. 2014;5:471.
- Neumar RW, Otto CW, Link MS, et al. Part 8: adult advanced cardiovascular life support: 2010 American Heart Association Guidelines for Cardiopulmonary Resuscitation and Emergency Cardiovascular Care. Circulation. 2010;122(18 Suppl 3):S729-S767.
- Pollock S, Reid H, Klapper P, Metcalfe RA, Ahmed N. Herpes simplex encephalitis presenting as the sick sinus syndrome. J Neurol Neurosurg Psychiatry. 1986;49(3):331-332.
- Kennedy PGE. Viral encephalitis: causes, differential diagnosis, and management. J Neurol Neurosurg Psychiatry. 2004;75 Suppl 1(Suppl 1):i10-15.
- Smith BK, Cook MJ, Prior DL. Sinus node arrest secondary to HSV encephalitis. J Clin Neurosci. 2008;15(9):1053-1056.
- Skelly MJ, Burger AA, Adekola O. Herpes Simplex Virus-1 Encephalitis: A Review of Current Disease Management with Three Case Reports. Antivir Chem Chemother. 2012;23(1):13-18.
- Ak AK, Bhutta BS, Mendez MD. Herpes Simplex Encephalitis. In: StatPearls [Internet]. StatPearls Publishing; 2024.
Braiman D, Konstantino Y, Westreich R. When the brain slows the heart—herpes encephalitis and sinus arrest: a case report. Eur Heart J Case Rep. 2021;5(8):ytab254.