



Up to 200,000 patients per year in the U.S. are given percutaneous endoscopic gastrostomy (PEG) tubes.
The PEG tube is indicated in many critically ill patients, including those with a limited ability to tolerate oral intake due to trauma or obstruction; PEG tubes may also be used for gastric decompression. However, a sizeable portion of those who receive PEG tubes struggle with dislodged tubes.
Case Presentation
A 72-year-old male with a history of left side deficit secondary to a previous stroke presented to the ED after pulling his trach and G-tube. The patient was oriented to self and place, and physical exam showed no bleeding or signs of infection around the site. However, the G-tube was pulled at least 3 hours prior to arrival. After 3 hours there’s concern for closure of the tract, even for an established G-tube.
Instead of attempting to open the tract with a Foley catheter, a bougie was used, as it is more rigid than the urinary drainage catheter. It was applied with gentle pressure to re-open the lumen, then replaced with a smaller G-tube. The follow-up x-ray with diatrizoate showed the G-tube in place within the body of the stomach and without contrast extravasation. There were no complications from the procedure.
Discussion
Accidental PEG tube dislodgement rates have been reported between 1% and 13.4% when followed longitudinally for the lifetime of the PEG, with some reports showing displacement in up to 20% of patients.1,2 A report in the Pennsylvania Patient Safety Authority described G-tube dislodgments as the most frequently reported complicated of G-tubes; one study revealed a rate of 78.3% displacement over 5 years. The report included potential causes of G-tube dislodgment, including the patient pulling on the tube and tube movement during patient care.3
As nursing home populations rise while a nursing shortage persists, the chance of a G-tube dislodgment occurring and going unnoticed in that setting increases. However, replacement of the tube is time-sensitive to prevent the tract from closing; some reports encourage replacement within a 2-hr window to prevent complications.3
Troubleshooting Dislodged Tubes
Historically, we have placed a Foley catheter in the stoma to keep it open until time allows for replacement of the tube. After determining the length of time the tube has been in place, the length of time it’s been dislodged, and performing an abdominal exam, replacement of the tube can take place.
One other piece of equipment can be considered in managing dislodged PEG tubes: the bougie. There are no formal studies concerning the efficacy or complication rate of using a bougie to keep the PEG stoma open. In some cases, the Foley catheter may not access the stoma once it’s started closing. EMDocs recommends attempting access with red rubber catheters, curved forceps, or an irrigation syringe to widen the stoma. However, it’s never been recommended to use a bougie.4 The bougie provides enough flexibility to receive positive feedback from surrounding structures while simultaneously incorporating enough rigidity to prevent rolling on itself.5 In contrast, the Foley catheter method frequently doesn’t work, may cause trauma to the site, or coil on itself.
Conclusion
Due to the rigidity, availability, and size of the bougie, it makes an excellent option for G-tube replacement and tract dilation in the setting of delayed G-tube replacement requiring a downsized tube.
In recent experience it has had a 100% success rate in a small sample size in various community emergency departments within the Texas area, including several nursing home patients who may not have the knowledge or equipment readily available to keep the tract patent in a timely manner.
Image 1. Endotracheal tube introducers and airway exchange catheters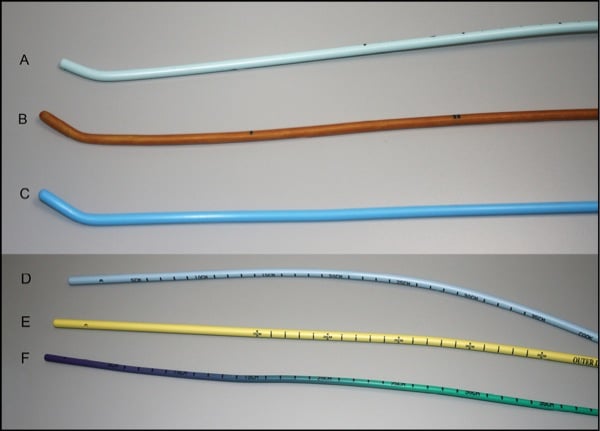
(A) Portex single-use introducer (Smiths Medical); (B) the reusable Eschmann tracheal tube introducer (Portex Venn, Smiths Medical); (C) gum-elastic bougie (SunMed); (D) Cook Medical Aintree intubation catheter; (E) Cook airway exchange catheter; (F) Cook airway exchange catheter (Image courtesy of Anesthesia News)
References
- Billington M, Young N, Mackey M, Donaldson CR, Lu K. Displaced G-tube. WikiEM. 2023.
- Rosenberger LH, Guidry CA, Davis JP, Hranjec T, Johnston VK, Wages NA, Watson CM, Sawyer RG. Reducing Accidental Dislodgement of the Percutaneous Endoscopic Gastrostomy: A Prospective Trial of the "SafetyBreak" Device. Surg Innov. 2015;23(1):62-69.
- Feil M. Dislodged gastrointestinal tubes: preventing a potentially fatal complication. Pa Patient Safety Advis. 2017;14(1):9-16.
- Herman L. 2016. Troubleshooting G-tubes and J-tubes: common scenarios/tips & tricks. emDocs. 2016.
- Intersurgical complete respiratory systems. Universal Stylet Bougie. 2024.