



The Case
A 48-year-old female with no contributing past medical history presented to the emergency department with her left index finger trapped in the gas filler cap valve of a vehicle.
History of Present Illness
The patient was attempting to inspect the gas filler area of her vehicle when her left index finger became lodged in the gas filler cap valve. Despite multiple attempts to free the finger, including the use of lubrication, Detroit emergency medical services were unable to extricate the finger and sought assistance.
The Detroit Fire Department was called to the scene and initially attempted to cut open the gas access door and pipe to facilitate removal. Despite these efforts, the finger remained trapped, leading to her transfer to the Henry Ford Hospital emergency department for further intervention.
Figure 1. The patient arrived to the ED with her left index finger stuck in the gas filler cap valve. Sterile gauze tied to an IV pole was used to stabilize the patient and machinery to facilitate inspection.
Physical Examination
The left index finger was swollen, tender to palpation, and visibly trapped within the gas filler valve. There was worsening pain with any attempt to free the finger by attempting to open the filler valve. The left radial pulse was able to be easily palpated, and all soft tissue compartments of the finger, hand, and proximal left upper extremity were soft. The gas filler valve and finger were carefully inspected with flashlight and, ultimately, fiber-optic nasopharyngeal scope. Endoscopic evaluation showed the gas cap valve itself was tightly secured around the finger on the hinge side.
Figure 2. The view of the patient's hand entering the gas filler cap
Figure 3. An external view of the left index finger exiting the gas filler cap to be stuck within the valve mechanism
Considered Interventions
Digital nerve block was deferred in order to preserve frequent re-assessment of the finger’s neurovascular status, particularly in the setting of anticipated heat-generating removal procedure. There was also concern that performing a digital nerve block could worsen swelling and possibly make the finger more difficult to extricate or possibly precipitate compartment syndrome over time with further swelling from the injury. The patient responded well to serial doses of morphine and midazolam while finger was entrapped.
Failed Interventions
- Lubrication: Initial attempts to free the finger in the field using lubrication, such as with petroleum jelly, were unsuccessful. As the patient's finger was stuck in the hinge mechanism of the gas filler cap valve, which was not known until later endoscopic visualization in the emergency department, lubrication and attempts at opening the gas filler cap valve were unsuccessful.
- Bougie and Suture Removal: In the emergency department, prior to endoscopic visualization, running a bougie and suture through the gas filler cap valve were attempted to better open the valve to facilitate extrication. As above, this method failed due to the nature of the entrapment.
- Operating Room Equipment: The patient’s case was discussed with orthopedic surgery regarding any OR equipment that could help facilitate freeing the finger. After discussion, it was determined that their bolt cutters and bone saws would not be effective to extricate the finger.
Successful Interventions
- Endoscopic Visualization: An endoscopic approach was utilized to better understand the nature of the entrapment. A fiber-optic nasopharyngeal scope was inserted into the gas access pipe and advanced until the finger and valve were visualized, revealing that the tip of the finger was trapped in the valve hinge. This visualization allowed for a more precise understanding of the entrapment mechanics and explained why previous attempts were unsuccessful and often led to worsening pain experienced by the patient.
- Angle Grinder Utilization: Due to the persistent nature of the entrapment and the failure of previous methods, an angle grinder was employed to cut through the gas access pipe connecting to the gas filler cap valve. The facilities department at the hospital was initially unreachable in the search for an angle grinder. Local hardware stores in downtown Detroit did not stock angle grinders, and nurses who lived nearby did not have one at home. The Detroit Fire Department would not agree to return to the ED to allow us to use their angle grinder. It was decided to use DoorDash to facilitate delivery of an angle grinder or a reciprocating saw. While DoorDash was en route, a facilities employee brought an angle grinder to the ED. This approach was chosen to facilitate safe and effective removal of the finger. The procedure was conducted with mild sedation to minimize discomfort. After the gas access pipe was cut, the gas filler cap valve hinge was cut with wire cutters, and the finger was freed from the gas tank.
Figure 4. Endoscopic visualization with a flexible fiberoptic nasopharyngeal scope reveals the finger to be caught in the hinge mechanism of the valve
Procedure Details
The gas access door and pipe were carefully cut from the rest of the car by the Detroit Fire Department in the field to allow access to the gas filler cap valve. In the emergency department, the angle grinder was used to precisely cut and remove sections of the gas access pipe, creating sufficient space to visualize the finger in the gas filler cap valve, and the finger was subsequently freed by cutting the valve hinge with wire cutters. The procedure was performed under unsterile conditions and was performed 3 hours past the initial entrapment time, allowing for volatile gasoline vapors to be eliminated. Wet towels were used to protect the patient from sparks. Extra wet towels were available in case of fire, which was low risk. Saline was applied to the cutting surface via IV tubing to minimize heat production. The gas filler cap valve and finger were carefully examined post-removal for any residual debris or damage.
Figure 5. An angle grinder was used to cut the gas access pipe. Wet towels were used to protect the patient and staff, and saline was applied via IV tubing to decrease heat production
Figure 6. After cutting the gas access pipe, easy access was obtained to the patient’s finger within the gas filler cap valve
Figure 7. A focused image of the patient’s finger within the gas filler cap valve hinge after the gas access pipe was cut
Figure 8. The hinge of the gas filler cap valve was cut with wire cutters, was removed, and the hand is subsequently visualized to be within the gas filler cap
Post-Procedure Care
The patient’s finger was cleaned, and an ice pack was applied to reduce swelling. Post-procedural x-ray was negative for fracture, dislocation, and radio-opaque foreign body. The finger was bandaged and closely monitored for signs of infection or further complications during the remainder of the patient's emergency department stay. Pain management and follow-up care instructions were provided to the patient, including monitoring for signs of infection and changes in sensation.
Outcome
The patient experienced relief following the procedure and showed no immediate complications. The patient signed consent for publication purposes and was lost to follow up.
Figure 9. The gas filler cap and gas access pipe are shown after removal from the patient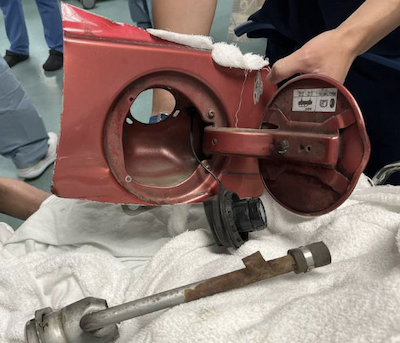
Figure 10. The patient’s finger is visualized immediately after freeing from the gas filler cap valve
Discussion
This case illustrates the complexity of managing severe entrapment incidents involving automotive components. The use of an angle grinder, while effective, underscores the need for a methodical approach and readiness to employ advanced techniques when initial interventions fail. Endoscopic visualization played a crucial role in identifying the exact nature of the entrapment, guiding the subsequent treatment strategy.
Conclusion
The patient’s severe entrapment was successfully managed through a combination of emergency services and advanced medical techniques. The case highlights the importance of a comprehensive approach in handling complex entrapment scenarios and the need for both initial and advanced intervention strategies.
Take-Home Points
- Need for increased public and provider awareness regarding safety measures when interacting with automotive components
- Training for emergency responders regarding handling unusual entrapment situations with appropriate tools and techniques
- Use of fiber-optic nasopharyngeal scopes to better visualize and diagnose entrapment situations
- Creative resource utilization such as hospital facilities, employee personal tools, and delivery services
- Fire safety when performing heat and spark generating procedures near hospital oxygen and gasoline fumes