



A 22-year-old male with a history of sickle cell disease is brought to the ED by police after he was found altered and naked outside on a rainy night.
What is your interpretation of the following ECG?
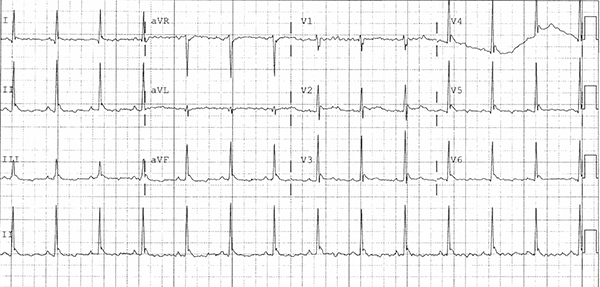
J Waves (Osborn waves)
This EKG shows a normal sinus rhythm with a ventricular rate of 80, a normal axis, and early R-wave transition in the precordial leads. There is diffuse T-wave flattening and some baseline artifact that makes calculating the QTc difficult, but it prolonged when measured in V2. J waves, also called Osborn waves, are present in leads V2-V6 and the inferior leads.
J waves are positive deflections at the terminal junction of QRS and beginning of the ST-segment takeoff resembling a dome or hump.1 They are often seen in the hypothermic patient and the amplitude and duration have been shown to correlate with the degree of hypothermia. They are most commonly seen in the inferior (particularly lead II) and lateral precordial leads but can be seen in any or all leads depending on the degree of hypothermia.
In 1953, Dr. John Osborn described J waves as an “current of injury” concerning for impending ventricular fibrillation in the setting of hypothermia.2 Although J waves had been reported before this in hypercalcemia and hypothermia, the J wave became known as the Osborn wave as a testament to his work. There is no consensus on which name to use, and some use Osborn wave when seen with hypothermia and J wave in all other settings.
Despite Dr. Osborn’s research, the association of J waves with life-threatening dysrhythmias in the hypothermic patient is unclear. As well, the presence of J waves is not pathognomonic for hypothermia. J waves can be seen with hypercalcemia,3 cardiac ischemia, and CNS injury (eg, SAH). There is even a case report describing J waves in the setting of Todd’s paralysis.4 Accordingly, the presence of J waves on an ECG warrants a broad differential diagnosis, including environmental exposure, cardiac ischemia, electrolyte abnormalities, and neurologic pathology.
Learning Points
ECG Findings in Hypothermia

General Features
- Findings most commonly seen at < 32°C
EKG Features
- Bradydysrhythmias
- Atrial fibrillation with slow ventricular rate
- Sinus bradycardia with 1st degree AV block
- Junctional rhythms
- Prolongation of PR, QRS, and/or QT intervals
- J waves (also called Osborn waves)
- Positive deflection at the terminal junction of QRS and beginning of the ST-segment takeoff (see Figure)
- Most commonly seen in the inferior and lateral precordial leads
Clinical Significance
- Amplitude and duration of J waves typically correlate with the degree of hypothermia
- J waves can also be seen with hypercalcemia and intracranial hemorrhage
Case Conclusion
The presence of J waves made us concerned about hypothermia, and the patient’s core temperature was found to be 29.5°C. His workup was notable for multiple traumatic injuries. The patient was placed on a rewarming protocol and transferred to the Surgical ICU for further management of his traumatic injuries.
For more details about pacemaker malfunctions, see pages 55-56 of the EMRA EKG Guide.
References
1. Gussak I, Bjerregaard P, Egan TM, Chaitman BR. ECG phenomenon called the J wave. History, pathophysiology and clinical significance. J Electrocardiol. 1995;28(1):49-58.
2. Osborn JJ. Experimental hypothermia; respiratory and blood pH changes in relation to cardiac function. Am J Physiol. 1953;175(3):389-398.
3. Morales GX, Bodiwala K, Elayi CS. Giant J-wave (Osborn wave) unrelated to hypothermia. EP Europace. 2011;13(2):283.
4. O’Connell E, Baker N, Dandamudi G, Steinhubl S. Dynamic J-Point Elevation Associated with Epileptic Hemiplegia: The Osborn Wave of Todd’s Paralysis. Case Rep Neurol. 2013;5(1):6-9.