



While only about 4% of patients with pulmonary embolism (PE) present with hemodynamic instability or cardiac arrest (CA), evidence shows that up to 65% of massive PEs are fatal.7
Current Advanced Cardiovascular Life Support (ACLS) and American Heart Association (AHA) guidelines suggest thrombolytics should be considered for cardiac arrest due to presumed PE.
There have been no randomized control trials (RCTs) that have studied the administration of thrombolytics in cardiac arrest due to PE. The only RCTs that added information involved administering thrombolytics in undifferentiated cardiac arrest, and they did not show a survival benefit.
This deep dive evaluates the existing evidence to help inform your practice. (Click here for the downloadable Powerpoint deck.)
RCTs looking at thrombolytics in undifferentiated cardiac arrest (not specific to PE)
Abu-Laban RB, Christenson JM, Innes GD, et al. Tissue plasminogen activator in cardiac arrest with pulseless electrical activity. N Engl J Med. 2002;346(20):1522-1528.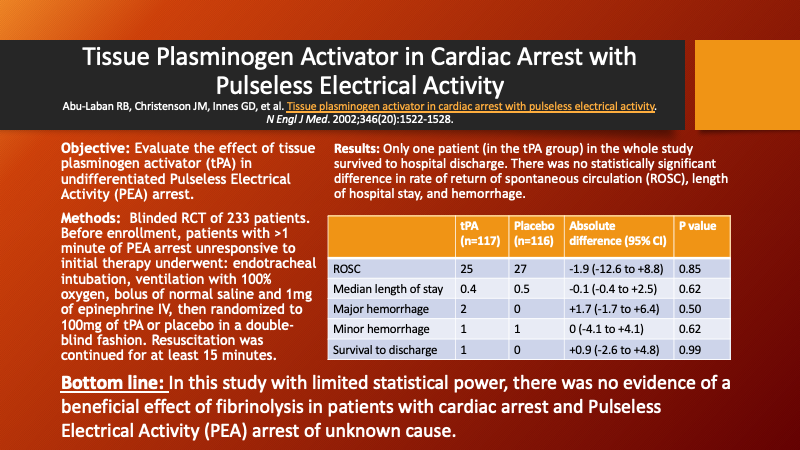
Böttiger BW, Arntz HR, Chamberlain DA, et al. Thrombolysis during resuscitation for out-of-hospital cardiac arrest. N Engl J Med. 2008;359(25):2651-2662.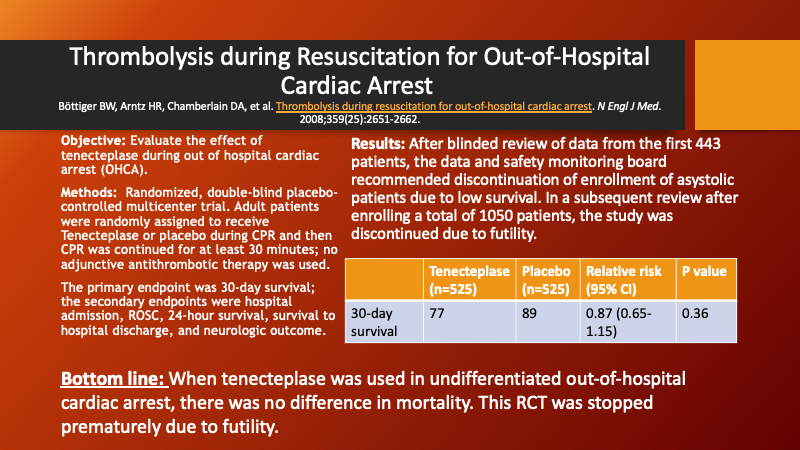
Evidence specific to cardiac arrest from presumed PE (none are RCTs)
Sharifi M, Berger J, Beeston P, et al. Pulseless electrical activity in pulmonary embolism treated with thrombolysis (from the "PEAPETT" study). Am J Emerg Med. 2016;34(10):1963-1967.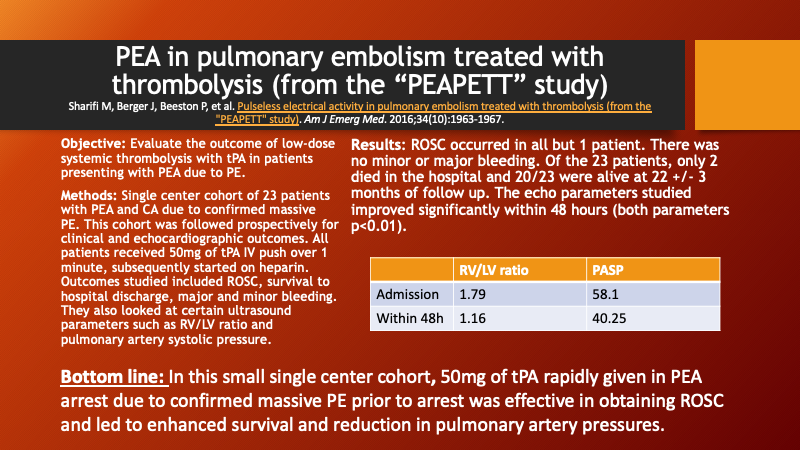
Yousuf T, Brinton T, Ahmed K, Iskander J, Woznicka D, Kramer J, Kopiec A, Chadaga AR, Ortiz K. Tissue Plasminogen Activator Use in Cardiac Arrest Secondary to Fulminant Pulmonary Embolism. J Clin Med Res. 2016 Mar;8(3):190-5.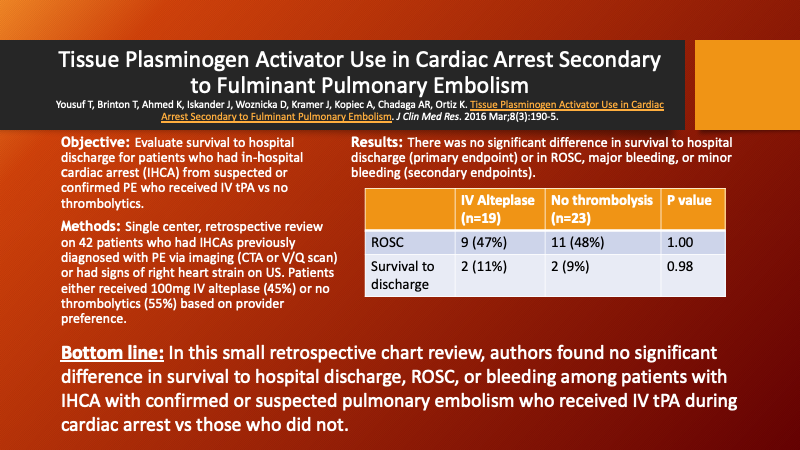
Peppard SR, Parks AM, Zimmerman J. Characterization of alteplase therapy for presumed or confirmed pulmonary embolism during cardiac arrest. Am J Health Syst Pharm. 2018 Jun 15;75(12):870-875. doi: 10.2146/ajhp170450.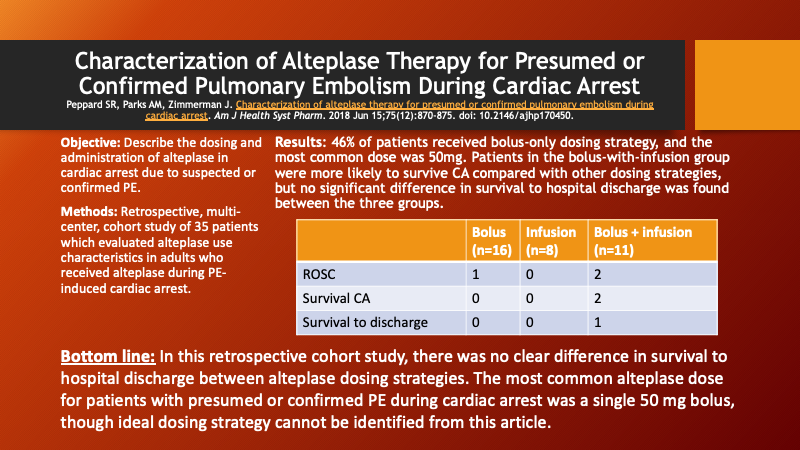
Summers K, Schultheis J, Raiff D, Dahhan T. Evaluation of Rescue Thrombolysis in Cardiac Arrest Secondary to Suspected or Confirmed Pulmonary Embolism. Ann Pharmacother. 2019 Jul;53(7):711-715.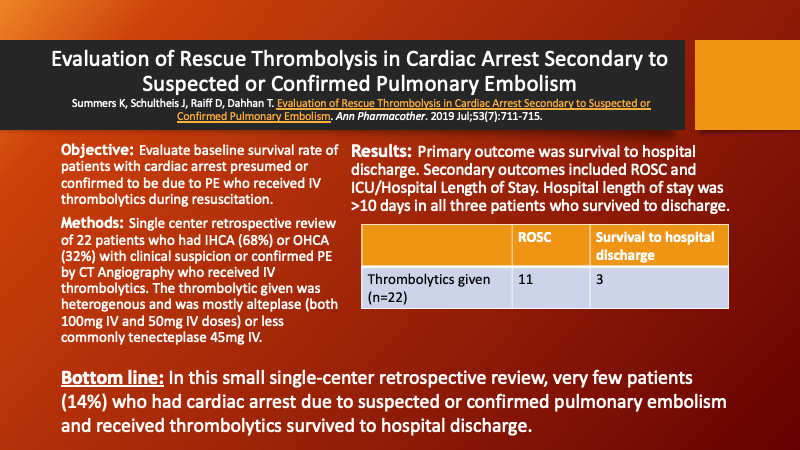
de Paz D, Diez J, Ariza F, Scarpetta DF, Quintero JA, Carvajal SM. Emergency Thrombolysis During Cardiac Arrest Due to Pulmonary Thromboembolism: Our Experience Over 6 Years. Open Access Emerg Med. 2021 Feb 22;13:67-73.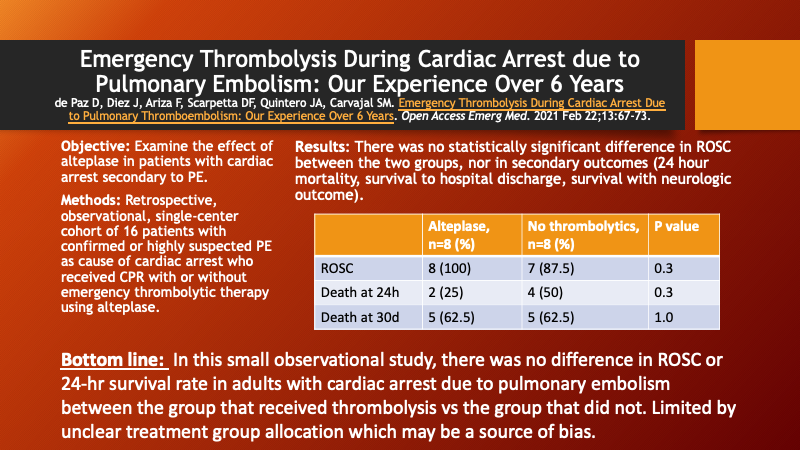
TAKE-HOME POINTS
- Few patients who suffer cardiac arrest from massive pulmonary embolism will survive to hospital discharge. There are a limited number of studies currently on use of thrombolytics for cardiac arrest due to pulmonary embolism, none of which are RCTs.
- From the evidence available, there is no clear mortality or functional outcome benefit to any IV thrombolytic in this patient population. Additionally, while alteplase is the most common thrombolytic, there is significant heterogeneity in the dosing strategies.
- It is important for the clinician to weigh the potential benefits of IV thrombolytics for each individual patient against the risk of rare but significant bleeding events.
- No strong conclusions can be made without further studies.
References
- Abu-Laban RB, Christenson JM, Innes GD, et al. Tissue plasminogen activator in cardiac arrest with pulseless electrical activity. N Engl J Med. 2002;346(20):1522-1528. doi: 346/20/1522 [pii].
- Böttiger BW, Arntz HR, Chamberlain DA, et al. Thrombolysis during resuscitation for out-of-hospital cardiac arrest. N Engl J Med. 2008;359(25):2651-2662. doi: 10.1056/NEJMoa070570 [doi].
- de Paz D, Diez J, Ariza F, Scarpetta DF, Quintero JA, Carvajal SM. Emergency thrombolysis during cardiac arrest due to pulmonary thromboembolism: Our experience over 6 years. Open Access Emerg Med. 2021;13:67-73. doi: 10.2147/OAEM.S275767 [doi].
- Dirican A, Ozkaya S, Atas AE, Ulu EK, Kitapci I, Ece F. Thrombolytic treatment (alteplase; rt-pa) in acute massive pulmonary embolism and cardiopulmonary arrest. Drug Des Devel Ther. 2014;8:759-763. doi: 10.2147/DDDT.S61679 [doi].
- Igneri LA, Hammer JM. Systemic thrombolytic therapy for massive and submassive pulmonary embolism. J Pharm Pract. 2020;33(1):74-89. doi: 10.1177/0897190018767769 [doi].
- Javaudin F, Lascarrou JB, Le Bastard Q, et al. Thrombolysis during resuscitation for out-of-hospital cardiac arrest caused by pulmonary embolism increases 30-day survival: Findings from the french national cardiac arrest registry. Chest. 2019;156(6):1167-1175. doi: S0012-3692(19)31390-X [pii].
- Logan JK, Pantle H, Huiras P, Bessman E, Bright L. Evidence-based diagnosis and thrombolytic treatment of cardiac arrest or periarrest due to suspected pulmonary embolism. Am J Emerg Med. 2014;32(7):789-796. doi: S0735-6757(14)00276-9 [pii].
- Long B, Koyfman A. Current controversies in thrombolytic use in acute pulmonary embolism. J Emerg Med. 2016;51(1):37-44. doi: S0736-4679(16)00150-5 [pii].
- Niwa A, Nakamura M, Harada N, Musha T. Observational investigation of thrombolysis with the tissue-type plasminogen activator monteplase for acute pulmonary embolism in japan. Circ J. 2012;76(10):2471-2480. doi: N/JST.JSTAGE/circj/CJ-12-0091 [pii].
- Nobre C, Thomas B, Santos L, Tavares J. Prolonged chest compressions during cardiopulmonary resuscitation for in-hospital cardiac arrest due to acute pulmonary embolism. Tex Heart Inst J. 2015;42(2):136-138. doi: 10.14503/THIJ-14-4267 [doi].
- Peppard SR, Parks AM, Zimmerman J. Characterization of alteplase therapy for presumed or confirmed pulmonary embolism during cardiac arrest. Am J Health Syst Pharm. 2018;75(12):870-875. doi: 10.2146/ajhp170450 [doi].
- Peters NA, Paciullo CA. Alteplase for the treatment of pulmonary embolism: A review. Adv Emerg Nurs J. 2015;37(4):258-72; quiz E4. doi: 10.1097/TME.0000000000000082 [doi].
- Sharifi M, Berger J, Beeston P, et al. Pulseless electrical activity in pulmonary embolism treated with thrombolysis (from the "PEAPETT" study). Am J Emerg Med. 2016;34(10):1963-1967. doi: S0735-6757(16)30351-5 [pii].
- Summers K, Schultheis J, Raiff D, Dahhan T. Evaluation of rescue thrombolysis in cardiac arrest secondary to suspected or confirmed pulmonary embolism. Ann Pharmacother. 2019;53(7):711-715. doi: 10.1177/1060028019828423 [doi].
- Yousuf T, Brinton T, Ahmed K, et al. Tissue plasminogen activator use in cardiac arrest secondary to fulminant pulmonary embolism. J Clin Med Res. 2016;8(3):190-195. doi: 10.14740/jocmr2452w [doi].