



Cuff defects top the list of structural causes of air leak from endotracheal tubes. Being able to troubleshoot the problem without changing the ETT decreases risk to the patient and saves valuable time.
A 59-year-old male with a history of Type II diabetes and hypertension presents to the emergency department with greater than 50% body surface area burns, shortness of breath, and stridor after being trapped in a confined space on fire. The patient has third-degree burns of his entire face, scalp, and anterior neck. He is obtunded, tachycardic, tachypneic with respirations of 28-32, and marked stridor on inspiration, as well as an oxygen saturation of 90% on non-rebreather face mask at 15 LPM. On examination of the mouth and nose there are singed nasal hairs, erythematous oral mucosa with secretions, and soot visible in the posterior oropharynx.
The decision is made to emergently intubate the patient as a result of his inability to protect his airway, respiratory distress, and anticipated swelling of his airway secondary to burns. Equipment is prepared, medications are drawn up, the patient is successfully preoxygenated with oxygen saturations approaching 99%, and other interventions for effective burn resuscitation are completed. After appropriate RSI medications are administered a senior resident attempts intubation but encounters difficulty because of profound soft tissue swelling in the posterior oropharynx. An experienced attending is able to successfully place in the endotracheal tube (ETT), with position confirmation by equal bilateral breath sounds, quantitative waveform capnography, and chest X-ray.
Several minutes later, the team is called back to the bedside by a respiratory therapist who has identified a substantial cuff leak of the ETT resulting in inadequate ventilation of the patient. A quick evaluation of the tube reveals a damaged pilot balloon line causing cuff deflation. The team is concerned about removal of the tube, even using bougie, Aintree, or other device to exchange the tube, given the difficulty with initial intubation and severe, progressive soft tissue swelling.
What can be done to repair the pilot line?
Literature Review
A malfunctioning ETT pilot balloon or pilot line (either incompetent valve, damage to balloon, or damage to the pilot line) might lead to inability to ventilate because of a large leak. Changing the ETT can prove challenging in certain clinical scenarios (eg, full stomach patient, difficult airway, or prone position). Being able to troubleshoot the problem and avoid changing the ETT decreases the risk to the patient and saves time.
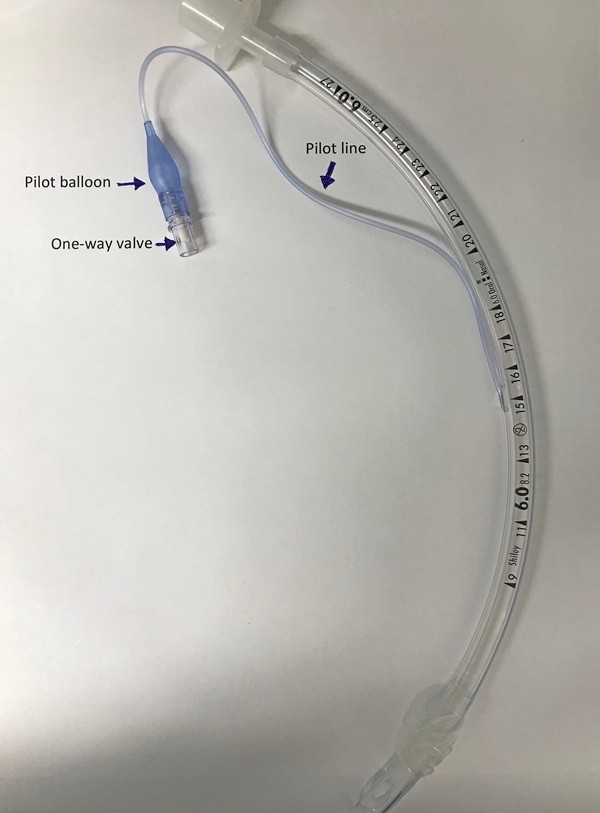
Figure 1. Anatomy of an endotracheal tube
Cuff defects top the list of structural causes of air leak from endotracheal tubes.1 Damage to the cuff during tube insertion, especially during multiple intubation attempts, on teeth or hardware in the mouth is often the culprit.2 Also, damage can occur as a result of inadvertent contact with other medical equipment such as needles, scalpels, or forceps.3 Even application of local anesthetic to the cuff material has been implicated in cuff defects sufficient to cause a leak.4
If the cuff itself is damaged, the only viable solution to reestablish a secure airway is to change the tube.1 However, damage to the pilot line or pilot balloon may be repairable without having to exchange the tube.
Cases of pilot balloon and pilot line failure, although rarer, also have been reported previously in the anesthesia, critical care, and EM literature. The one-way inflation valve of the pilot balloon can be incompetent as a result of poor manufacturing, mechanical trauma, or even routine use of connecting an air syringe to inflate the cuff.5 The pilot balloon, much like the cuff, can be torn, punctured, or otherwise damaged on teeth or sharp equipment, causing leakage of air or failure to inflate altogether.6,7 Likewise there have been reports of the pilot tubing being damaged by tube securing devices, accidently cut, or faulty manufacturing.8,9
Other techniques for pilot line and pilot balloon repair have been described, but often require specialized equipment. Ideally, one would be able to acquire a commercially available repair kit.10 However, these are not readily stocked in every ED. Rao et al. described a novel, improvised way of fixing an ETT pilot line with a Portex epidural connector.11 While anesthesia colleagues may have easy access to this device, it is not a common piece of equipment in the ED. Other techniques such as using an IV catheter and stopcock setup11,12,13 or even a hypodermic needle in various configurations14,15 have been proposed. These solutions may be more feasible given the equipment available to prehospital and ED providers.
Techniques in the ED or Prehospital Environment
Here are 4 easy techniques with equipment readily available in any ED, operating room, intensive care unit, or ambulance to fix the leak and avoid changing the ETT.
Situation No. 1. The one-way valve malfunctions, but the pilot balloon and line are intact.
Attach a T-piece connector or a clave to the pilot balloon, and then inflate with a syringe. Clamp the T piece with a hemostat or IV tubing clamp, and disconnect the syringe.
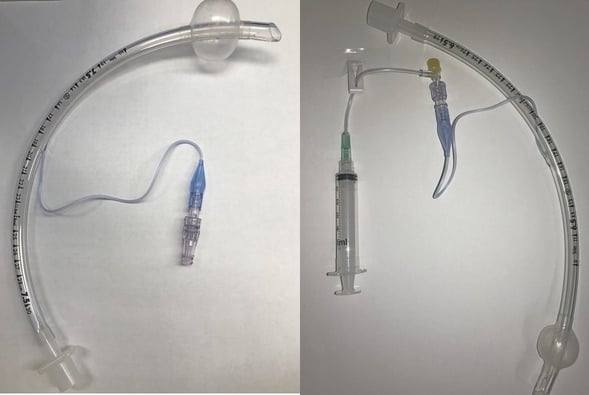
Figure 2 (left) showing clave technique and Figure 3 (right) showing IV extension tubing technique for repairing a faulty pilot balloon valve
Situation No. 2. The pilot balloon or pilot line is ruptured.
Cut the line below the break. Insert either a blunt needle or a 22G catheter into the lumen of the line. Connect it to a syringe and inflate the cuff. Clamp the line, and cover needle or catheter with a transparent film dressing or clave.

Figure 4 (left) showing catheter technique and Figure 5 (right) demonstrating needle technique for damaged pilot balloon or pilot balloon line
Case Resolution
A resident on the team quickly grabs a 22 gauge IV catheter, clave, 10 cc syringe, and TegadermTM from the IV access cart in the resuscitation room. She quickly identifies the site where air is leaking from the pilot line. With her trauma shears, she cuts the line just beyond leak, proximal to the cuff. Then, she removes the plastic 22 gauge catheter from the IV needle and inserts it snugly into the open end of the pilot line. A clave is attached to the end of the catheter and a 10 cc syringe is connected. The cuff is then successfully reinflated, with cessation of the air leak and return of effective ventilation. Finally, the TegadermTM is wrapped around the pilot line, catheter, and clave to ensure an airtight connection.
TAKE-HOME POINTS
Cuff leak from damage to an ETT cuff, pilot line, pilot balloon, or valve can cause inadequate ventilation and presents a significant patient safety issue with an unsecure airway.
While damage to the ETT cuff itself necessitates replacement of the tube, equipment failure proximal to cuff in the pilot line, pilot balloon, or valve can be easily fixed.
A faulty valve can be repaired with a clave for IV extension tubing.
A leaking pilot line or pilot balloon can be repaired by first cutting distal to the site of damage, then using a conduit such as a 22 ga catheter or blunt needled to reinflate the balloon, and finally prevent egress of air by clamping or otherwise occluding the pilot line.
References
1. Kearl RA, Hooper RG. Massive airway leaks: an analysis of the role of endotracheal tubes. Crit Care Med. 1993;21(4):518-21.
2. Verborgh C, Camu F. Management of cuff incompetence in an endotracheal tube. Anesthesiology. 1987;66(3):441.
3. Klipper WS, Waite HD, Tomlinson CO. Endotracheal Cuff Perforation Complicating Subclavian Venipuncture. JAMA. 1974;228(6):693.
4. Walmsley AJ, Burville LM, Davis TP. Cuff failure in polyvinyl chloride tracheal tubes sprayed with lignocaine. Anaesthesia. 1988;43(5):399-401.
5. Heusner JE, Viscomi CM. Endotracheal tube cuff failure due to valve damage. Anesth Analg. 1991; 72(2): 270.
6. Malhotra N, Singhal S. Slow deflation of a tracheal tube cuff: an unusual cause. Acta Anaesthesiol Scand. 2006; 50: 519–20.
7. El-Orbany M, Salem MR. Endotracheal Tube Cuff Leaks: Causes, Consequences, and Management. Anesth Analg. 2013; 117(2): 428.
8. Gupta B, Farooque K, Jain D, Kapoor R. Improper tube fixation causing a leaky cuff. J Emerg Trauma Shock. 2010; 3(2):182-184.
9. Gettelman TA, Morris GN. Endotracheal Tube Failure: Undetected by Routine Testing. Anesth Analg. 1995;81(6):1313.
10. Tri-anim Health Services. Pilot Tube Repair Kit, Endotracheal and Tracheostomy Tubes, Single Patient Use. https://www.tri-anim.com/pilot-tube-repair-kit-endotracheal-and-tracheostomy-tubes-single-patient-use-pharm-30993-3797.aspx. Accessed January 12, 2019.
11. Rao AK, Chaudhuri S, Joseph TT, Kamble D, Gotur G, Venkatesh S. Severed cuff inflation tubing of endotracheal tube: A novel way to prevent cuff deflation. Anesth Essays Res. 2014;8(2):243-246.
12. Watson E, Harris MM. Leaking endotracheal tube. Chest. 1989;95:709.
13. Kovatsis PG, Fiadjoe JE, Stricker PA. Simple, reliable replacement of pilot balloons for a variety of clinical situations. Ped Anesth. 2010;20(6):490-4.
14. Sprung J, Bourke DL, Thomas P, Harrison C. Clever cure for an endotracheal tube cuff leak. Anesthesiology. 1994;81:790-791.
15. Sills J. An emergency cuff inflation technique. Respir Care. 1986;31:199–201.