Ch 8. Subspecialty: Urban Search and Rescue
Goals
The objective of USAR is to recover casualties in a manner that maximizes the chance of recovery to their previous state of health and to rescue the highest number of people in the shortest amount of time while minimizing the risk to the rescuers.
Challenges
In confined spaces, special techniques are required to evalu- ate and treat the entrapped victim before extrication. Scoop and run philosophy is not possible with the trapped or pinned indi- vidual. The most important medical intervention in this setting is the prevention of cardiac complications and renal failure due to crush injury or crush syndrome. Stabilize patients prior to extrication if the scene is safe.
Characteristics of Confined Space Medicine
Confined spaces offer limited access and egress, along with unfavorable environmental conditions. Temperature extremes make hypothermia and hypoglycemia common; IV fluids and oxygen should be warmed. Confined spaces also contribute to heat-related illness, particularly for rescuers (protective clothing, strenuous activity, confined space, limited fluid intake). Encour- age breaks with liberal hydration.
Crush Injury/Crush Syndrome
The most dangerous time during a casualty is during the ex- trication phase when compressive forces are suddenly released. Prolonged, continuous pressure involving skeletal muscle mass results in muscle breakdown, and the subsequent release of muscle contents into the circulation results in renal failure and eventual cardiac arrest. Death can occur a few minutes after the casualty is freed. The deceptive feature of crush syndrome is that it does not develop until the limb is free from entrapment. Adverse effects do not occur until circulation is restored to mus- cles when the crushing object is lifted. Rehydration, rewarming, and bicarbonate must be started prior to the complete extrica- tion. Anticipate large amounts of IV fluid (6-10L) in the immedi- ate post-release period.
Pulmonary Concerns
Airway obstruction, particulate contamination, restriction of ventilation, inhalation injury, and blast lung are the main con- cerns. Crush injury to the chest can be fatal and is not a com- mon cause of death in collapse casualties. Particles from building collapse may induce acute and chronic pulmonary toxicity, pri- marily with the inflammatory and fibrogenic effects, and by inju- ry to the cellular defense mechanism of the lung.
Volume Concerns and Vascular Access
Trapped victims are subject to dehydration, hemorrhage, and third spacing. Early fluid administration is important to prevent delayed complications as the victim is freed from the rubble.
Vascular access must be initiated as soon as possible.
Timing Is Everything
Urban search and rescue uses the concept of “the golden day.” The chance of extricating a casualty alive drops dramat- ically after 24 hours. However, there are reports of casualties surviving after being entrapped for 6 days and longer. Efforts should not be delayed or abandoned after 24 hours.
- 30 minutes — 91.0% survive
- 1 day — 81.0% survive
- 2 days — 36.7% survive
- 3 days — 33.7% survive
- 4 days — 19.0% survive
- 5 days — 7.4% survive
FEMA (Federal Emergency Management Agency)
FEMA, an agency of the U.S. Department of Homeland Secu- rity, promotes an emergency response based on small, decentralized teams trained in areas of the National Disaster Medical System (NDMS), Urban Search and Rescue (USAR), Disaster Mor- tuary Operations Response Team (DMORT), Disaster Medical Assistance Team (DMAT), and Mobile Emergency Resource Support (MERS). If there is a disaster warranting USAR support, local emergency manager may request assistance from state or the state may request federal assistance. FEMA will deploy the three closest task forces within 6 hours of notification.
Task Forces
The team should be self-sufficient for a minimum of 72 hours before needing to resupply and should have a capability to operate for at least 10 days before personnel replacement is needed. The team is also responsible for bringing its own rescue equipment, support materials, and medical equipment.
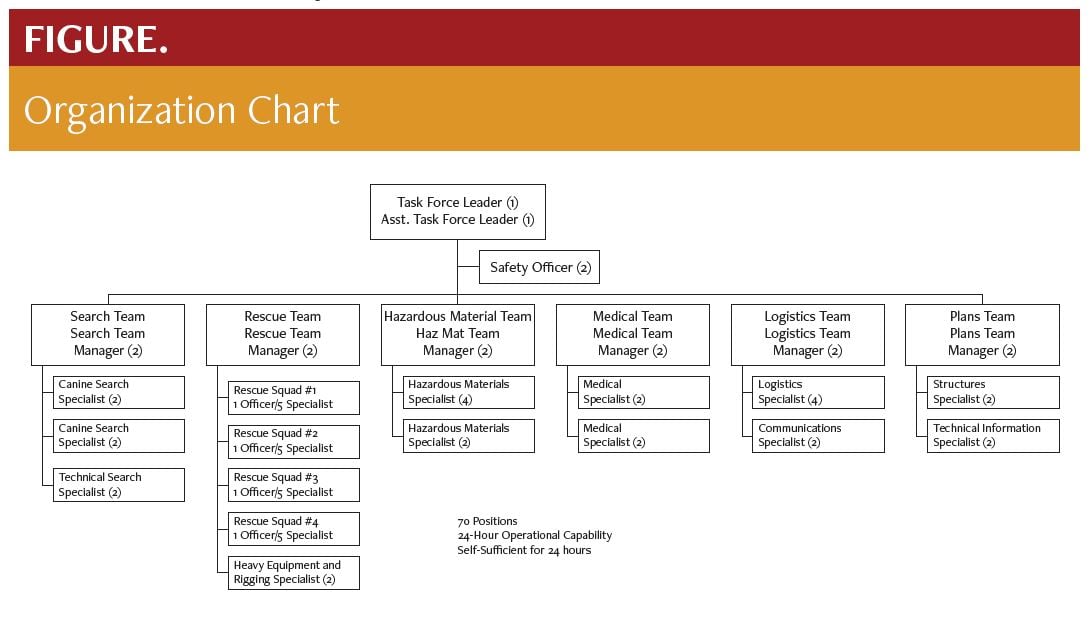
Organization Chart
Task Force Leader - Blend the team into the incident com- mand structure of the local authorities and other agencies for implementation of their tactical assignment.
Search Team - Locate casualties using canines, special proto- cols, and equipment.
Rescue Team - Evaluate the collapsed structure, stabilize the structure, and extricate casualties.
Technical Team - Hazardous materials assessment, structural stabilization, advice, communications, liaison for the local sys- tem, and logistical management.
Medical Team - Provides sophisticated emergency medical care for a potentially prolonged period during a mission. Unlike traditional disaster field care, such as that provided under a disaster medical assistance team (DMAT), the USAR medical team is designed to deliver more sophisticated care to fewer patients. The team must be medically self-sufficient and must not rely on the local medical system for support.
Treatment Priorities
After the care of the task force is ensured, attention can be turned to entrapped casualties, search team canines, and the surrounding community. The USAR medical team will hand casu- alties over to local EMS agencies or DMAT at a designated loca- tion just outside the perimeter of the working rescue zone.
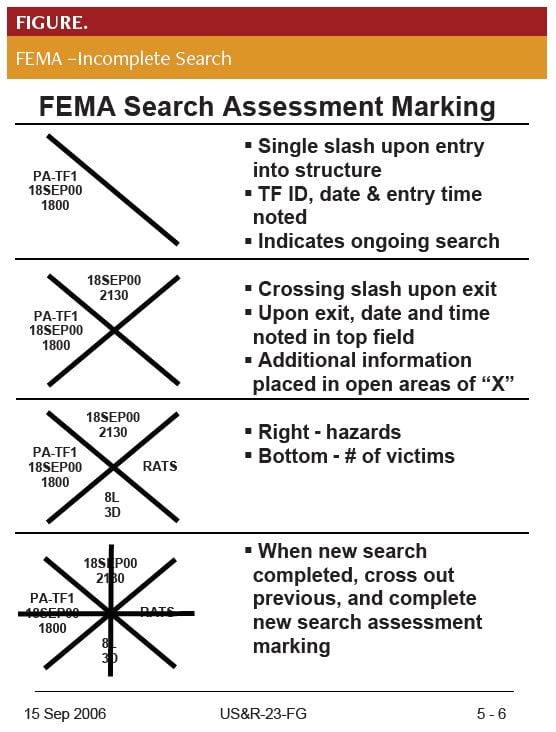
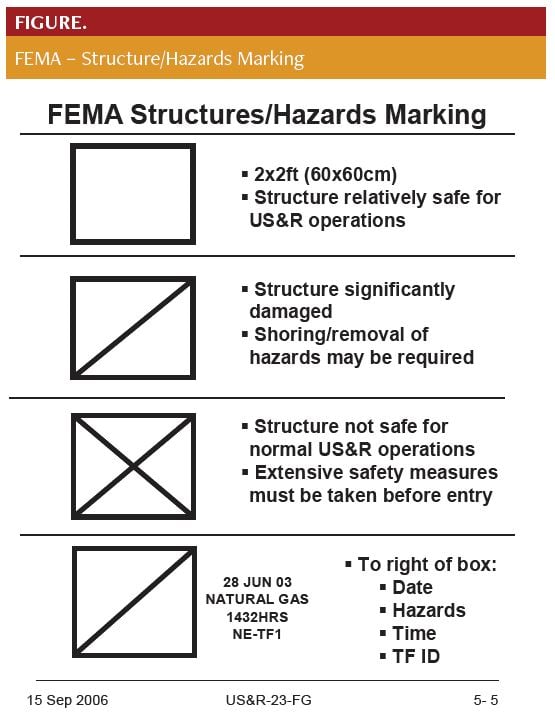
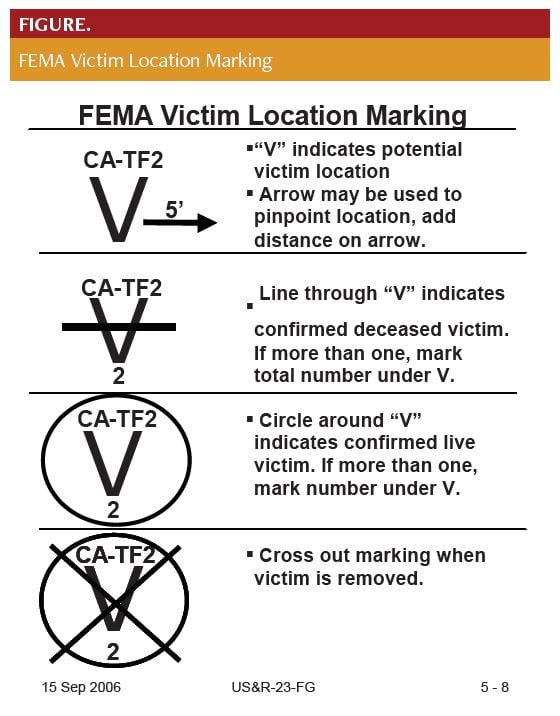
United States FEMA Markings
The structure triage, assessment, and marking system is de- signed to help identify, select, and prioritize the buildings with the highest probability of success with respect to finding and rescuing live victims. It is important that information related to building identification, conditions and hazards, and victim status be posted in a standardized fashion.
A 2x2 square box is outlined at any entrance accessible for en- try into a compromised structure.
Aerosol spray cans (International orange color only) are used for the marking system.
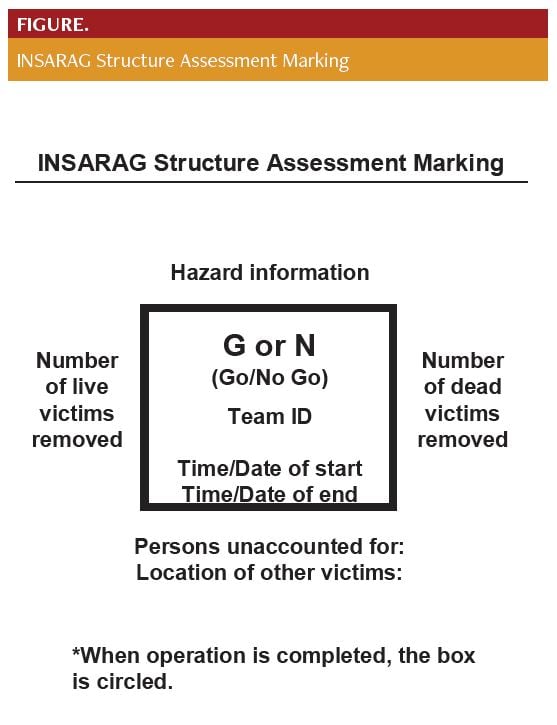
International Search and Rescue Advisory Group (INSARAG)
INSARAG is a global network of disaster-prone and disas- ter-responding countries and organizations dedicated to USAR
and operational field coordination. It aims to establish standards and classification for international USAR teams as well as methodology for international response coordination in the aftermath of earthquakes and collapsed structure disasters. The INSARAG Secretariat is located in the United Nations Office for the Coor- dination of Humanitarian Affairs (OCHA).
References
- Goodman C, Hogan, D. Urban Search and Rescue. In: Hogan D, Burstein, J, eds. Disaster Medicine. Philadelphia: Lippincott Williams and Wilkins; 2002:112-122.
- National Urban Search & Rescue Response System’s Rescue Field Operations Guide. https://www.fema.gov/pdf/emergency/usr/usr_23_20080205_rog.pdf.