




Ch 14. Subspecialty: Water Rescue
Water rescue is any incident that involves the removal of victims from any body of water other than a swimming pool. Floods are the most common of all natural disasters and gener- ally cause greater mortality than any other natural hazard.
Hazards Associated with Water Rescue
- Human nature: The “need to do something now” can prompt people to make rescue attempts without proper training or equipment.
- Environmental: Hazards can involve extreme temperatures; cold affects ability to think clearly and hampers fine motor skills; heat exhaustion and dehydration are a concern as well.
- Weather: Accelerates hypothermia. In still water body heat is lost 25 times faster than in air at the same temperature.
- Aquatic environment: Be aware of animal life, fish, insects, plant life, seaweed, biohazards, bacterial, and viral risks.
- Dive option hazards: These include barotrauma, decompression sickness, nitrogen narcosis, oxygen toxicity, embolism, fatigue, loss of air, anxiety reactions.
- Ice operation hazards: Cold injuries such as frostbite or hypothermia; thin ice with sudden immersion reflex or entrapment under ice.
- Swift water operation hazards: Strainers and debris, holes, obstructions above or below the water surface.
Safety of a Rescuer – “Throw, Don’t Go”
Jumping in the water to rescue a victim is the last resort. Avoid getting into a dangerous situation. Your safety is priority.
Water Rescue PPE
Wet suits/dry suits/exposure suits Thermal protection
PFDs include a whistle, knife, strobe light, or light stick worn by all personnel in or near water or on a boat
Lifelines, helmet, gloves
Rescue Plan of Action & Methods
First unit on scene sizes up the situation and determines the number and condition of patients. If rescue is deemed necessary, consider the need for additional personnel and equipment.
Secure the immediate area to prevent an increase of victims.
Assess hazards, location, and number of victims. Before com- mencing extraction, yell clear and simple instructions to the victim. Ensure firm footing and remember the victim is in duress and may pull rescuers into the water.
REACH
Step 1: Reach with an outstretched arm, leg, or other tool (long stick/scarf/clothes) from a crouched or lying position.
- DO NOT enter water any deeper than knee deep, unless tethered.
WADE
Step 2: Test the depth with a long stick before wading in and then use the stick to reach out. Hold on to someone else or the bank.
THROW
Step 3: Throw rope bags, life rings, and floats - anything that will float (this is only effective when the subject is cooperative)
ROW
Step 4: Use a boat if you can use it safely. Do not try to pull the person on board in case they panic and capsize the boat.
Continuously monitor situations that could adversely affect the rescue, such as a rise in water, top loads, suspended loads, or shifting of rescue vehicle.
Once the victim has been removed to a safe area, medical personnel should be on scene to evaluate and transport to the hospital if necessary.
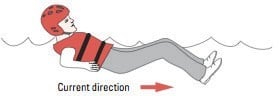
Safe Swimming Position
If you get swept away, assume the safe swimming position and navigate with ferry angle. (Image)
Awareness Level Personnel (Resident) may:
- Establish scene controls.
- Establish Incident Command.
- Initiate accountability and safety.
- Evaluate patient condition.
- Activate needed resources.
- Secure and interview witnesses.
- Establish last seen point.
- Identify number of victims, age, and sex of victims.
Sectorization of Rescue Operation
Upstream group: Responsible to watch for and advise of any obstacles and hazards that may hinder the rescue operation.
Downstream group: Prepare to rescue victims and rescu- ers that may be swept downstream. All members in this group should have a throw rope bag in hand and deploy on both sides to the bank.
River right/left group: Responsible for rigging the opposite end of a rope rescue system.
Rescue group: Responsible for developing an action with command. Once action plan has been developed, rescue group will execute plan in the safest possible manner.
Medical group: Responsible for providing first aid treatment to victims removed from the water.
Rescue Communications
Whistle Commands
- 1 Blast = Stop and look at me
- 2 Blasts = Begin the action that we agreed upon or is indicated
- 3 Blasts (repetitive) = I need help
Hand Signals
- One arm in air = I need help
- One hand on top of head = I am OK Rope Signals
- 1 Tug = OK
- 2 Tugs = Advance
- 3 Tugs = Take up slack 4 Tugs = Help
Technique for Mechanical Advantage
Vector pull: By attaching one end of the rope to an anchor and the other to the pinned object, the rope can then be pulled near the mid-point in a sideways direction to exert a much great- er force on the pinned object.
Z drag/pulley system: Theoretical mechanical advantage of 3, giving a 3:1 haul ratio. Requires excess gear, time, and only pulls the pinned object 1 foot for every 3 feet pulled by the user.
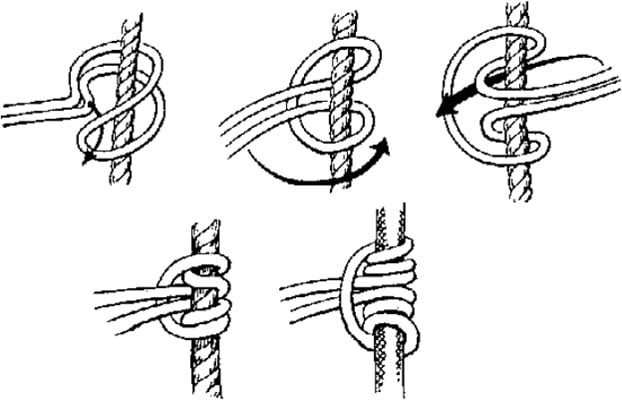
Prusik 1 provides the mechanical advantage.
Prusik 2 can be used to hold the position of the rope.
Prusik knot slides easily along a tight rope but jams solidly upon loading.
Drowning
Drowning is a process resulting in primary respiratory impairment from submersion or immersion in a liquid medium. The distinction between salt water and fresh water drowning is no lon- ger important in non-fatal drowning. Both result in hypoxia and pulmonary edema. Panic causes loss of normal breathing pattern and reflex inspiratory efforts, followed by aspiration and reflex laryngospasm, hypoxemia, end organ damage, and death.
Management
Ventilation is priority, unlike in cardiac arrest. If the patient does not respond to 2 rescue breaths that make the chest rise, the rescuer should immediately begin performing high-quality chest compressions. CPR, including the application of an au- tomated external defibrillator, is then performed according to standard guidelines. Cervical spine immobilization is not recom- mended unless there are clinical signs of injury or concerning mechanism, as it can interfere with essential airway manage- ment.
Drowning patients can present with life-threatening arrhyth- mias. Treat according to ACLS protocols. Assess pulse for at least 1 minute before initiating chest compressions, as pulses may be weak in a hypothermic patient. Heimlich maneuver and postural drainage is no longer recommended.
Hypothermia
Hypothermia is a core temperature less than 35 Celsius. Water does not have to be ice-cold for hypothermia or other cold-relat- ed injuries. Most water is well below human core body tempera- ture. Prolonged exposure to water may result in hypothermia.
Generally, a hypothermic patient is never considered dead until the core temperature is increased to 32º Celsius.
Mild hypothermia: Core temperature 32-35º C (90-95º F); result is tachypnea, tachycardia, initial hyperventilation, ataxia, dysarthria, impaired judgment, shivering, and cold diuresis.
Moderate hypothermia: Core temperature 28-32º C (82-90º F); proportionate reductions in pulse rate and cardiac output, hypoventilation, central nervous system depression, hyporeflexia, decreased renal blood flow, and loss of shivering. Paradoxical undressing may be observed. Atrial fibrillation, junctional brady- cardia, and other arrhythmias can occur.
Severe hypothermia: Core temperature < 28º C (82º F); pul- monary edema, oliguria, areflexia, coma, hypotension, bradycar- dia, ventricular arrhythmias including ventricular fibrillation, or asystole occur.
References
- Giesbrecht GG, Hayward JS. Problems and complications with cold-water rescue Giesbert. Wilderness Environ Med. 2006;17(1):26-30.
- Orlowski JP, Szpilman D. Drowning. Rescue, resuscitation, and reanimation. Pediatr Clin North Am. 2001;48(3):627-646.
- Poole J, Hogan DE. Disaster Medicine – Floods. Wolters Kluwer Health. 2007
- Water Rescue Awareness – Pasco Fire Department
- Pendley T. The Essential Technical Rescue Field Operations Guide. 4th ed. 2003 Pendley.