



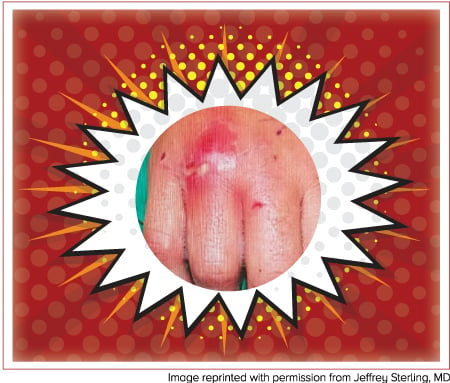
A 27-year-old male presents to the emergency department complaining of purulent drainage from a wound to his right hand. He says that he was in a fight about one week prior and punched another individual in the mouth during a night of drinking. His vital signs are within normal limits. On exam, he is noted to have a 1 cm laceration over the fourth metacarpophalangeal joint. There is localized erythema and swelling around the bite as well as thick, yellow drainage. Range of motion is limited by pain, and sensation is intact. What is your next step in management?
Background
Mammalian bites account for almost 1% of emergency room visits annually in the United States. Human bites are the third most common cause, only behind cat and dog bites.1 However, human bite wounds have a much higher incidence of infection and can cause serious complications if not treated appropriately.2
Human bites usually occur in one of two ways. A “fight bite” occurs when one person punches another person in the mouth with a clenched fist. An occlusive bite occurs when one human directly bites the tissue of another individual in an attempt to harm. These types of bites most commonly occur on the extremities or face. For bites that occur on the hand (such as in a fight bite scenario), harm is done when the tooth penetrates the capsule of the metacarpophalangeal joint. Bacteria from the mouth enter the joint but then become trapped as the fist is released from a clenched position.
At first, the bite wound usually appears innocuous. However, without treatment, severe complications may occur. These include local skin infections, lymphangitis, septic arthritis, tenosynovitis, tendon injury, fracture, osteomyelitis, or uncommon systemic complications such as bacteremia, endocarditis, or meningitis.3
Microbiology
Human bite wound infections tend to be polymicrobial, and organisms originate from both the oral cavity of the biter and from the skin of the bite victim.4 Staphylococcus aureus and alpha-hemolytic streptococci (eg, Viridans group streptococci) are the most common isolated organisms. Eikenella corrodens, a gram negative anaerobic bacillus, is also a frequent isolate.5 Other organisms include Bacteroides spp, Corynebacterium, and Fusobacterium spp.
Since hepatitis C virus (HCV) and human immunodeficiency virus (HIV) transmissions require blood exposure, and since saliva is usually blood-free, the risk of HCV-HIV transmission from a biter to a bitee is negligible. However, since a biter's oral mucosa invariably gets exposed to the victim's blood (reverse exposure), testing for HCV and HIV should be considered.5
Clostridium tetani is not commonly encountered in human bites, but it could potentially be transmitted via this pathway. Therefore, it is recommended that appropriate tetanus prophylaxis be administered.7
Treatment
Human bites almost always require antibiotics and fight bites always require an operating room. Unfortunately, many patients do not present immediately after the event because of the initial unassuming nature of the wound. Patients will often not present to a physician until after colonization by a number of microorganisms has already occurred and the wound starts to exhibit macroscopic signs of infection. The infection rate can be as high as 47% for any human bite that is not treated with antibiotics.6
Radiographs are indicated in all cases in order to rule out any foreign objects, such as dislodged teeth.8 Imaging will also assist in ruling out fracture, and in chronic presentations, osteomyelitis.
Initial treatment involves copious irrigation and exploration. If a joint capsule or tendon is involved, it must be washed out and immobilized.8 All fight bites need to be taken to the operating room for irrigation and debridement of the wound and joint capsule. If the wound is located on a limb, without joint involvement, it is preferred to leave the wound open. The only exception is facial wounds, which may be closed for cosmetic reasons as long as there is no overt sign of infection after proper irrigation and examination. A surgery consultation is recommended for the following:3
— Fight bite
— Presence of necrotic tissue
— Osteomyelitis
— Tenosynovitis
— Foreign body
— Abscess
— Septic arthritis
— Nerve or vascular injury
Considering the high infection rate of human bites, antibiotics are given prophylactically whenever the wound penetrates the epidermis. If the wound is grossly infected, if systemic symptoms are present, or if the patient will be going to the operating room, they should receive intravenous antibiotics. The duration of antibiotic prophylaxis is 3-5 days, whereas treatment is 5-7 days (Table 1).
| Table 1. Human Bites9 |
| Key organisms: Viridans group streptococci, Bacteroides spp., Coagulase-negative staphylococci, Corynebacterium spp., S. aureus, Eikenella corrodens, Fusobacterium spp., Peptostreptococcus spp. |
| Treatment duration: 5-7 days, prophylaxis 3-5 days |
• Amoxicillin/clavulanate 875mg PO two times daily |
• Doxycycline 100mg PO two times daily |
• Moxifloxacin 400mg PO/IV once daily |
• Ampicillin/sulbactam 3g IV four times daily |
• Imipenem 1g IV four times daily |
Key Points
- Nearly half of human bite wounds will become infected if not treated with antibiotics.
- The goal should always be to prevent infection with proper wound irrigation, exploration, and antibiotic prophylaxis.
- Consult surgery for patients with fight bites, or any other wound complications.
Acknowledgements
We would like to thank Josh Bucher, MD (Assistant Professor, Rutgers – RWJMS Department of Emergency Medicine) for his help proofreading the article.
References
- Nakamura Y, Daya M. Use of Appropriate Antimicrobials in Wound Management. Plast Reconstr Surg. 1991;88:111-114.
- Seppanen, M. Bite Wounds. EBM Guidelines, Duodecim Medical Publications Ltd, 11/2015.
- Patil PD, Panchabhai TS, Galwankar SC. Managing human bites. J Emerg Trauma Shock. 2009;2(3):186-190.
- Brook I. Management of Human and Animal Bite Wounds: An Overview. Adv Skin Wound Care. 2005;18(4):197-203.
- Ghan-Shyam L, Lillia T, Sapna L, Sunita L. Human bites: Bloodborne pathogen risk and post-exposure follow-up algorithm. J Natl Med Assoc. 2013;105(1):92-95.
- Isaacs, L. Antibiotic Treatment Essential for Human and Animal Bites. EM News. 2004;26(13):16,18.
- Kretsinger K, Broder KR, Cortese MM, et al. Preventing tetanus, diphtheria, and pertussis among adults: use of tetanus toxoid, reduced diphtheria toxoid and acellular pertussis vaccine recommendations of the Advisory Committee on Immunization Practices (ACIP) and recommendation of ACIP, supported by the Healthcare Infection Control Practices Advisory Committee (HICPAC), for use of Tdap among health-care personnel. MMWR Recomm Rep. 2006;55:1-37.
- Staiano J, Graham K. A Tooth in the hand is Worth a Washout in the Operating Theater. J Trauma. 2007;62(6):1531-1532.
- Ahlers E, Phelan P. Animal/Human Bite Wounds. In: Levine B, ed. EMRA Antibiotic Guide. 17th ed. Irving, TX: EMRA; 2016:82-83.