



Case. A 59-year-old male smoker with a history of hypertension, familial hyperlipidemia and insulin dependent diabetes presents with 2 hours of substernal chest pressure radiating to his right arm.
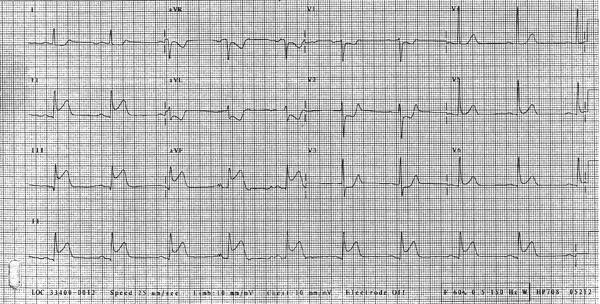
This ECG is clearly concerning for an ischemic event, with both ST elevations and ST depressions. As always we will approach this ECG in a systematic way to ensure the obvious findings don't obscure subtler findings.
First of all, this ECG demonstrates sinus rhythm with regular rate and normal axis. The PR interval is on the high end of normal, and the QTc is normal. The QRS complex is narrow and there are no delta waves in any lead. Significantly, there are ST elevations in the inferior leads (II, III, aVF) as well as ST depressions in aVL, V1, V2, V3. ST elevations in the inferior leads are concerning for inferior wall MI which usually occurs from RCA occlusion. These patients should not be given nitroglycerin as it may instigate hypotension. They are also at risk of developing bradycardia secondary to AV block. ST elevation is considered significant if there is at least 1 mm (one small box) of elevation at the J point in at least 2 contiguous leads except for the precordial leads (V2, V3) which require 2 mm of elevation to be significant.
The ST depressions in the anterior leads of this ECG should make you concerned for a posterior wall MI and should prompt a posterior ECG. This is especially concerning in the presence of upright T waves in these leads. ST depression in aVL (a lateral lead) is likely a reciprocal change from inferior ST elevations discussed above. Seeing this ECG should obligate an immediate consultation to the cardiology service and to the cardiac cath lab for possible stenting.
Learning Points
- ST elevation greater than 1 mm in 2 contiguous leads (2 mm in V2 and V3) should make you seriously entertain the diagnosis of STEMI in your patient and prompt immediate action to activate the nearest cardiac cath lab.
- Remember the PAILS mnemonic when assessing for reciprocal changes. PAILS stands for P-posterior A-anterior I-inferior L-lateral S-septal. ST elevations in these leads most commonly create reciprocal ST depressions in the corresponding leads of the next letter in the mnemonic. That is to say, posterior ST elevation will usually cause anterior lead ST depressions and anterior lead ST elevations will usually be seen with inferior lead depressions.
- Nitro should not be given in the presence of inferior wall ST elevations as it may induce hypotension. Inferior wall infarctions may also be associated with AV nodal dysfunction causing heart block and bradycardia.